Translate this page into:
Lichen planus affecting eyelid alone: A rare entity
Correspondence Address:
Shyam B Verma
B3, C.S. Patel Enclave 3, Pratapgunj, Baroda - 390 002
India
| How to cite this article: Verma SB. Lichen planus affecting eyelid alone: A rare entity. Indian J Dermatol Venereol Leprol 2006;72:398 |
Abstract
Lichen planus of the eyelid alone is a rarely reported condition with just about 11 cases reported so far in the international literature. We report a case of lichen planus of single lower eyelid with characteristic histopathologic findings on eyelid biopsy. It is unusual to encounter a usually characteristic and often widespread entity like lichen planus occuring at only one site like an eyelid. Lichen planus of the eyelid should be included in the differential diagnosis of eyelid dermatitis.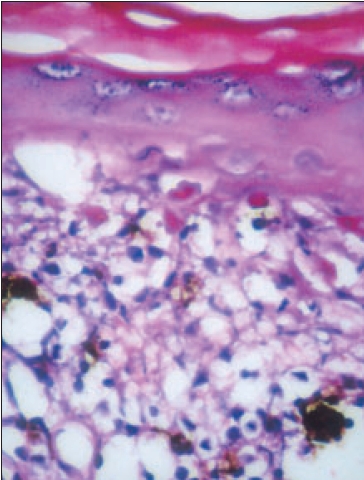 |
| Photomicrograph shows prominent Civatte bodies and pigment incontinence (H and E, 400x) |
|
| Photomicrograph shows prominent Civatte bodies and pigment incontinence (H and E, 400x) |
 |
| Violaceous, linear plaque of lichen planus on the lower eyelid. |
|
| Violaceous, linear plaque of lichen planus on the lower eyelid. |
Introduction
Lichen planus of eyelids alone is a rare phenomenon. Eyelids can be the only site of affliction of the disease. It can be confused with the more common dermatoses occurring in the palpebral region, namely contact dermatitis, seborrheic dermatitis, atopic dermatitis, etc. A case of lichen planus of the lower eyelid is being reported.
Case report
A 68-year-old woman presented in this clinic with history of severe itching over her left lower eyelid. She had noticed a reddish thickened area for the past eight months, which got progressively larger and itchier till it reached the present stage.
On examination the woman had a violaceous and thin linear plaque over the left lower eyelid skin adjacent to the lid margin. It did not encroach upon the intermarginal strip of the eyelid and spared the puncta of the lacrimal ducts. There was no scarring of the skin or the conjunctiva [Figure - 1]. There was minimal scaling in the lesion. There was no edema or discharge. The other eye was normal [Figure - 1]. At that point two diagnoses were considered, namely lichen planus and psoriasis. Examination of the entire cutaneous surface of the patient did not reveal any similar lesion elsewhere. Her scalp oral and vaginal mucosae were normal. She was in apparent good health with no complaints. Her routine hemogram, blood sugar and other relevant investigations were within normal limits. There was no history of any drug intake in the past two years. There was no history of applying anything locally like any eye medication, cosmetics or dyes.
She was sent to the ophthalmologist for a biopsy. Histopathology showed hyperkeratosis, hypergranulosis, vacuolar degeneration of basal cell layer, saw tooth elongation of rete ridges and a bandlike infiltrate. Civatte bodies and pigment incontinence were conspicuous [Figure - 2]. The clinical diagnosis of lichen planus of the eyelid was thus confirmed. Direct immunofluorescence was negative for discoid lupus erythematosus. She decided to take homeopathic treatment and was lost to follow-up.
Discussion
Many dermatological conditions can affect the eyelids, the so-called palpebral dermatoses. The commonest cause is allergic contact dermatitis of the eyelids.[1],[2] Other conditions affecting the eyelids include irritant contact dermatitis, atopic dermatitis, seborrheic dermatitis and xerotic eyes. Rare causes include connective tissue disorders like overlap syndromes, dermatomyositis, lichen planus, psoriasis, discoid lupus erythematosus and basal cell carcinoma.[1],[2],[3] Lichen planus of the eyelids is a very rare phenomenon with just about 11 cases reported in the international literature.[4],[5],[6] These lesions may appear just on the eyelids without involvement of the rest of the body like in our case, making it very difficult to diagnose. However, the histopathology was characteristic, allowing a confident diagnosis to be made. It is proposed that lichen planus be included in the differential diagnosis of various dermatoses with palpebral involvement.
| 1. |
Guin JD. Eyelid dermatitis: Experience in 203 cases. J Am Acad Dermatol 2002;47:755-65.
[Google Scholar]
|
| 2. |
Ayala F, Fabbrocini G, Bacchilega R, Berardesca E, Caraffini S, Corazza M, et al . Eyelid dermatitis: An evaluation of 447 patients. Am J Contact Dermat 2003;14:69-74.
[Google Scholar]
|
| 3. |
Tursen U, Oz O, Ikizoglu G, Kaya TI, Dusmez D. A case of lichen planus - lupus erythematosus overlap syndrome with eyelid involvement. Eur J Ophthalmol 2002;12:244-6.
[Google Scholar]
|
| 4. |
Sharma R, Singhal N. Lichen planus of the eyelids: A report of 5 cases. Dermatol Online J 2001;7:5.
[Google Scholar]
|
| 5. |
Itin PH, Buechner SA, Rufli T. Lichen planus of the eyelids. Dermatology 1995;191:350-1.
[Google Scholar]
|
| 6. |
Vogel PS, James WD. Lichen planus of the eyelid: An unusual clinical presentation. J Am Acad Dermatol 1992;27:638-9.
[Google Scholar]
|
Fulltext Views
2,887
PDF downloads
1,247





![[Figure - 1]](#fig_ijdvl_2006_72_5_398_27771_1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2006_72_5_398_27771_2.jpg){kind=link}