Translate this page into:
Lipoblastoma in an 8-year-old child: An atypical presentation of a rare tumor
2 Department of Dermatology, Hospital Rey Juan Carlos, Mostoles, Madrid, Spain
Correspondence Address:
A Nuno-Gonzalez
Department of Dermatology, Hospital Universitario Fundacion Alcorcon, Calle Budapest, CP 28922, Alcorcon, Madrid
Spain
| How to cite this article: Nuno-Gonzalez A, Vicente-Martin F J, de la Fuente E G, Lopez-Estebaranz J L. Lipoblastoma in an 8-year-old child: An atypical presentation of a rare tumor. Indian J Dermatol Venereol Leprol 2013;79:553 |
Sir,
Lipoblastoma is a very rare tumor arising from the immature white fat. It usually occurs in the extremities of infants. Although it grows rapidly and may reach a large size, it is benign. [1]
We report the case of an 8-year-old male who showed signs of a nodular lesion in the posterior cervical area. It was asymptomatic and had been growing for 7 months [Figure - 1]a. Ultrasonography revealed a 5 cm subcutaneous soft-tissue mass. The magnetic resonance imaging (MRI) showed a fat tumor; which was oval and encapsulated, measuring 48 mm × 13 mm × 37 mm [Figure - 1]b. We performed surgery and achieved a complete excision of the encapsulated tumor [Figure - 1]c and d. The pathological examination showed a nodular lesion with lobular appearance; the adipose tissue lobes were separated by septa of connective tissue of varying thickness [Figure - 2]a. There were two different areas: the most immature area, which had a myxoid appearance with spindle cells [Figure - 2]b; and the mature adipose tissue, which had small blood vessels and occasional lipoblasts. There were no atypical cells or mitosis [Figure - 2]c and d. With the clinical, radiological and histological findings we made the diagnosis of lipoblastoma. After 18 months, the patient remains asymptomatic without signs of recurrence.
 |
| Figure 1: (a) Posterior cervical area showing a nodular lesion without skin changes. (b) T1-weighted magnetic resonance imaging shows an encapsulated fat density subcutaneous lesion. (c) Surgery excision and lipoblastoma removal. (d) Surgical defect with clear plane of dissection; muscular fascia can be appreciated without evidence of the initial tumor |
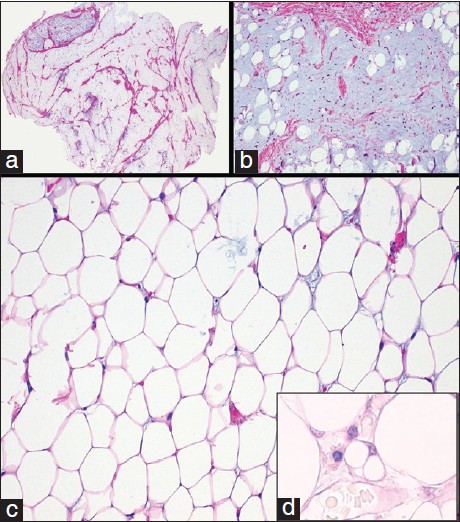 |
| Figure 2: (a) Fat tumor with fibrous septa and myxoid areas, predominantly in the periphery. Multinodular pattern is present, with adipose tissue lobes separated by septa of connective tissue of varying thickness (H and E, ×40). (b) Detail of the most immature area. It has a myxoid appearance with spindle cells (H and E, ×100). (c) Histological appearance of mature adipocytes (H and E, ×200). (d) Focal areas with lipoblasts (H and E, ×200) |
Lipoblastoma is a very rare tumor of embryonic fat. There are two different clinical forms; the encapsulated or lipoblastoma, and the diffuse, which is called lipoblastomatosis. This last form is associated with higher rates of recurrence after surgery. [2] Ninety percent of these cases occur in infants under 3 years of age, and up to 40% are younger than one. [1] Most of the cases are males, with a predominance of 3:1. Although, extremely rare, there have been cases reported in adults. [3] They are most common in the extremities, [4] occurring in 61% of the cases. Only 11% occur in the head and neck, [4] as in the case of our patient. Clinically, the differential diagnosis will be with lipoma, lymphangioma or myxoid liposarcoma. [1] Imaging tests are very important and the best technique is MRI, [4] which will usually show an encapsulated tumor with cystic areas and high-intensity signals on both T1-weighted and T2-weighted images. [5] The treatment of choice is surgical; but if a complete surgical approach is not possible, damaging adjacent structures is not justified, as lipoblastoma metastases have never been reported. [3]
The pathology will give us the final diagnosis: [3] a tumor composed of mature fat and myxoid changes with lipoblasts among the adipocytes. Sometimes, the differential diagnosis with myxoid liposarcoma can be very difficult, especially, when the patient is older, because lipoblastoma is very rare in children older than eight. [5] The pathological diagnostic clues to differentiate lipoblastoma from myxoid liposarcoma are that lipoblastomas are usually well encapsulated and lobulated, they have many mature cells, with no pleomorphism and atypia, and a small amount of vascularization compared to myxoid liposarcoma. In case of doubt, a cytogenetic analysis can help confirm the diagnosis. Most lipoblastomas have chromosome eight abnormalities such as translocations, deletions or duplications with secondary activation of oncogene PLAG1,on chromosome 8q 11-13 [3],[5] In summary, we present an atypical case of lipoblastoma because of the location of the tumor and the age of the child, highlighting the importance of imaging techniques and a proper surgical approach.
| 1. |
Pham NS, Poirier B, Fuller SC, Dublin AB, Tollefson TT. Pediatric lipoblastoma in the head and neck: A systematic review of 48 reported cases. Int J Pediatr Otorhinolaryngol 2010;74:723-8.
[Google Scholar]
|
| 2. |
Kok KY, Telisinghe PU. Lipoblastoma: Clinical features, treatment, and outcome. World J Surg 2010;34:1517-22.
[Google Scholar]
|
| 3. |
Coffin CM, Lowichik A, Putnam A. Lipoblastoma (LPB): A clinicopathologic and immunohistochemical analysis of 59 cases. Am J Surg Pathol 2009;33:1705-12.
[Google Scholar]
|
| 4. |
Akhtar T, Alladi A, Ahmed SM, Siddappa OS. Giant lipoblastoma of the thigh: A rare soft tissue tumor in an infant. J Cancer Res Ther 2012;8:157-8.
[Google Scholar]
|
| 5. |
Nagano A, Ohno T, Nishimoto Y, Hirose Y, Miyake S, Shimizu K.Lipoblastoma mimicking myxoid liposarcoma: A clinical report and literature review. Tohoku J Exp Med 2011;223:75-8.
[Google Scholar]
|
Fulltext Views
1,737
PDF downloads
1,826





![[Figure - 1]](#fig_ijdvl_2013_79_4_553_113115_u1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2013_79_4_553_113115_u2.jpg){kind=link}