Translate this page into:
Mesotherapy: What is new?
Correspondence Address:
Devinder M Thappa
Department of Dermatology and STD, JIPMER, Pondicherry-605 006
India
| How to cite this article: Konda D, Thappa DM. Mesotherapy: What is new?. Indian J Dermatol Venereol Leprol 2013;79:127-134 |
Introduction
"Mesotherapy" is a non-surgical, minimally invasive method of drug delivery that consists of multiple intradermal or subcutaneous injections of a mixture of compounds "melange" in minute doses. [1] Plant extracts, homeopathic agents, pharmaceuticals, vitamins and other bioactive substances can be used, but alcohol- or oil-based substances should not be used for mesotherapy because of the risk of cutaneous necrosis.
The term "mesotherapy" is derived from the Greek words "mesos" meaning "middle0" or "mean" and "therapeia" meaning "to treat medically," i.e. injecting into the middle layer of skin or "intradermotherapy." [2] The depth of penetration of the needle should not exceed 4 mm for it to be effective. [3]
Despite it being available for over 50 years and the huge publicity and attention received on the Internet, definite evidence for its efficacy is lacking and the claims are not always based on well-conducted clinical trials.
History
Mesotherapy for the first time was developed in 1952 by Dr. Michel Pistor, a French physician for the management of pain and vascular disorders. [4] Pistor coined the term "mesotherapy." He defined it as treatment of the mesoderm (the primary germ layer that develops into connective tissue, muscle and circulatory system). In 1976, he used the following words to describe mesotherapy: "little volume, few times and in the right place." [3]
Pistor founded the French Society of Mesotherapy in 1964 and, in 1987, The French National Academy of Medicine officially acknowledged mesotherapy as a medical specialty. [4] In the meantime, mesotherapy became popular in most parts of Europe and South America and, more recently, in the United States and Asian countries.
Indications of Mesotherapy
Mesotherapy, like corticosteroids, is claimed to have a wide array of applications especially in the field of cosmetic dermatology. However, only the current and widely practised indications in the field of dermatology along with the drugs used in them are discussed below.
- Body-cellulite, lipodissolve, body contouring (not very effective)
- Skin-rejuvenation/glow, lift, pigmentation
- Hair-telogen effluvium, androgenetic alopecia
Cellulite, local fat deposits and facial rejuvenation show good results with mesotherapy; telogen effluvium, androgenetic alopecia, stretch marks and facial pigmentation show moderate results; whereas body sculpting/contouring and melasma show doubtful results with the same.
An overview of the volume of cocktail to be injected, depth of penetration of mesotherapy needle and number of sessions needed for various uses is given below [5] [Table - 1].

Cellulite
Cellulite is an abnormal accumulation of fat above the fascia resulting in dimpling appearance of skin resembling an orange peel. [6] It is most commonly seen in the buttocks and thighs of females. It is seen in both normal and obese persons. It is believed to occur due to abnormality in the venolymphatic system. Therefore, accordingly, the cocktail solution for treatment of cellulite should contain the following agents: [6],[7]
Lipolytic : L-carnitine, caffeine, isoproterenol, thyroxine
Venostatic : rutin, aminophylline, pentoxiphylline
Drainage : Artichoke, gingko biloba
Anesthetic: procaine (also improves circulation)
Connective tissue breakdown : collagenase, hyaluronidase.
However, mesotherapy will be effective only when combined with proper diet and exercise.
Thyroid hormones are recently being used as a part of injection cocktails to cause reduction in fat. [8] They activate the sympathetic system and thus cause lipolysis by activating beta receptors. One case of thyrotoxicosis was reported after using cocktail containing tri iodothyronine
Localised fat deposits/lipo dissolve/injection lipolysis (chin jowls, double chin, eyepad fats)
Phosphatidyl choline (PC) and deoxycholate (DOC) are the most widely used agents for lipodissolve. PC is an antioxidant derived from soy lecithin. Depth of injection varies from 6 mm to 12 mm at a dose of 250 mg. [5] PC, however, cannot be used for the treatment of cellulite, which is a superficial condition.
PC, extracted from soybean lecithin (a) penetrates the adipocytes and breaks down fat, which is then carried to the blood stream and then excreted via the kidneys and bowel. [1] PC is viscous and, therefore, to facilitate its injection, an emulsifying agent, deoxycholate, is added, which is shown to independently cause lysis of the adipocytes. [9] (b) Promotes lipolysis by stimulating β receptors and inhibiting α2 receptors present on the adipocyte membrane, [10] (c) Also causes inflammatory cytokine-mediated necrosis and resorption of adipocytes. Once the inflammation subsides, new collagen is formed, leading to retraction of the loosened tissue. [11] Various substances used are: [6],[7]
Lipolytic : DOC (bile salt), L-carnitine (also causes fatty acid oxidation), aminophylline, caffeine, xanthine and organic silicium (also inhibits free radical formation, regenerates elastin and collagen)
Connective tissue breakdown : hyaluronidase, collagenase
Drainage enhancers : artichoke
Circulatory enhancers : yohimbine (α2 adrenergic blocker), aminophylline, pentoxiphylline.
Vitamin A and trace elements are important in regulating the turnover, keratinization and repair of keratinocytes; [6],[7] vitamin C enhances the synthesis of collagen and reduces hyperpigmentation as it inhibits melanin production; vitamin E, an antioxidant, aids in anti-aging of the skin; vitamin K affects clotting mechanisms and thus regulates the microcirculation of the skin.
A randomized, prospective case-controlled study over a 12-week period by Park et al.[12] to study the effect of a mixed solution (i.e., aminophylline, buflomedil and lidocaine) by injecting it into the superficial dermis of the medial aspect of the thigh weekly with the other thigh acting as a control showed no significant loss of thigh girth on the treated side as compared with the non-treated thigh as measured by computed tomographic scanning. The study indicated poor patient satisfaction and demonstrated that mesotherapy is not an effective alternative treatment modality for body contouring.
Mesolift/Mesoglow/Biorejuvenation
Mesolift/mesoglow is the term used for skin of face and neck rejuvenation. Agents [6],[7],[13] commonly used for mesolift are
Hyaluronic acid (HA): glycosaminoglycan, which binds and retains water thus improving the tone and elasticity of the skin. HA used in mesotherapy is not cross-linked (as the main function is to hydrate) in contrast to fillers, where it is cross-linked (as main function is to fill the gap and so need to be stabilised).
Multi vitamins, trace elements : ionic balance of the skin.
Amino acids, vegetal proteins : protein reconstruction.
Dimethylaminoethanol : precursor of PC, converts choline to acetylcholine (Ach) and thus causes muscle contraction leading to muscle firmness (mainly for lower face).
Hexapeptide 3 : blocks the Ach release [13] and thus relax the muscles and smoothens the wrinkles (mainly for the upper face).
Recently, natural/native freeze-dried collagen sheets are being used over the face after mesolift. Collagen sheets take up the shape of part of the face where it is applied and, due to its water retaining ability, hydrates and makes the skin firm. [14] Advantages being less post-procedure bruise, swelling and discomfort.
Ultrasound of the skin is used to evaluate the so-called subepidermal low echogenic band (SLEB), located immediately below the epidermal entrance echo as a marker of photo ageing. [15] It was seen that there was improvement in SLEB with mesotherapy. This can be explained by the hydrating effect of HA in the tissue due to its ability to absorb water many times its normal weight. [15] In addition, repeated injections into the dermis also can trigger the healing process, activating fibroblasts, producing more collagen.
However, a recent study [16] showed that mesotherapy injection of cocktail-containing multivitamin solution and non-cross-linked hyaluronic acid did not result in any significant clinical improvement and histological effects, which were assessed by quantitatively evaluating changes in collagen types 1, 3 and 7; elastin and tropoelastin (using immunohistochemistry) were also statistically insignificant.
Mesobotox
It involves multiple injections of small doses of botulinum toxin into the dermis (to create a dermal papule) to relax the superficial orbicular muscles of the face and reopen the sebaceous and sweat gland orifices thus increasing the glow of the skin. In this technique, the patient is asked to frown, purse the lips, give an exaggerated smile and raise eyebrows to make the desired muscle prominent, and then the injections are given according to mesotherapy principles. [17] Botulinum toxin (100 units) is mixed with physiological saline (1 mL, 5 mL, 7 mL) and xylocaine to make different concentrations. Concentrated toxin is to be used in thick and short muscles and diluted toxin in thin and flat muscles to avoid excess diffusion.
Alopecia
There are very few studies throwing light on the role of mesotherapy in treating alopecia. In a recent study conducted by Moftah et al., [18] it was seen that mesotherapy with dutasteride-containing preparation was significantly effective in female pattern hair loss rather than 0.9% saline after 16 weeks of treatment by four methods of assessment: photographic assessment, hair pull test, measurement of the hair diameter and patient self-assessment.
Scanning electron microscopic examination of the hair shaft showed the reappearance of the cuticle in two patients in whom it was focally destructed prior to the treatment. [18] However, there are few reports showing "alopecia" as a side-effect following the use of mesotherapy for alopecia. [19] Two patients developed patchy alopecia after mesotherapy, using heparinoid vasodilator mesoglycan in one patient and homoeopathic agents in the second patient. [20] Multifocal scalp abscess with subcutaneous fat necrosis and scarring alopecia were reported as complications of scalp mesotherapy. [21]
Despite the fact that there are no controlled published studies on mesotherapy′s efficacy in hair diseases, injections of minoxidil, finasteride, lidocaine, multivitamins and T3/T4 are used in the treatment of alopecia.
Cutaneous Leishmaniasis
Recently, mesogun is also used to deliver meglumine antimoniate into the lesions of cutaneous leishmaniasis. [22] This method had equal efficacy and was a comparatively less painful procedure when compared with the classical intralesional method.
Other Rare Uses
Mesotherapy is also tried in melasma, striae, vitiligo, hyperpigmentation, psoriasis, eczema and acne to minimize wrinkles and tighten loose skin.
Platelet-rich plasma in mesotherapy
A small amount of blood is withdrawn from the patient and centrifuged at a high speed and the platelet concentrate is injected intradermally into the scalp for scalp mesotherapy. [23] Growth factors and healing proteins from the platelets improve circulation to the hair follicles, causing hair follicle growth and thus causing hair growth.
Growth factors like platelet-derived growth factor, transforming growth factor and vascular endothelial growth factor released from alfa granules of the platelets increase the proliferation of fibroblasts, production of procollagen type 1 carboxy peptide by the dermal fibroblasts and thus improves the structural integrity of the skin. [24] This property enables platelet-rich plasma (PRP) to be used in photoaged and aged skin. PRP also induces the expression of matrix metalloproteinases, which break down and remove the collagen fragments that interfere with new collagen formation in aged skin. [23] Thus, PRP helps in remodelling of the skin. However, further studies are needed to ensure the safety of PRP as a component of mesotherapy.
Usually done once in every 4-6 months for 1 year, then every year as maintenance therapy depending on the patient′s response.
Peptides in mesotherapy
Acetyldecapeptide-3: reduces and prevents lines and wrinkles by actively generating new skin cells.
Decapeptide-4: for anti-aging and wound healing
Copper tripeptide-1: helps blood circulation in the skin and revitalises
Oligopeptide-24: minimises scars on skin by forming new skin cell
Tripeptide-6: hydrates dry skin and maintains its optimum moisture balance
And, others like, pentapeptide, L carnitine and licorice. Because of the above-mentioned properties, biopeptides [25] are an important component of mesolift, mesoglow, mesocellulite and mesohair and mesosculpting
Growth factors and stem cells in mesotherapy
Thymosin TB-4, a growth factor, is injected into the mesoderm of the scalp, i.e. directly into the hair foliclles as a part of scalp mesotherapy. [26],[27] TB-4 causes the growth of hair follicles by improving the circulation, stimulating the stem cells and reviving hair follicles.
Stem cells obtained from bone marrow are an important component of whitening serum and de-wrinkling solutions because of their proliferative capacity. [26],[27] Stem cells are now an important component of whitening solutions.
Various mixtures and protocols in mesotherapy
Materials used in mesotherapy can be broadly classified into two categories: [6],[7],[12],[28]
- Principal (P)/major
- Complementary (C)/minor
Cocktail or the mixture should contain at least two to three principal agents for it to be effective.
Procedure and injection techniques
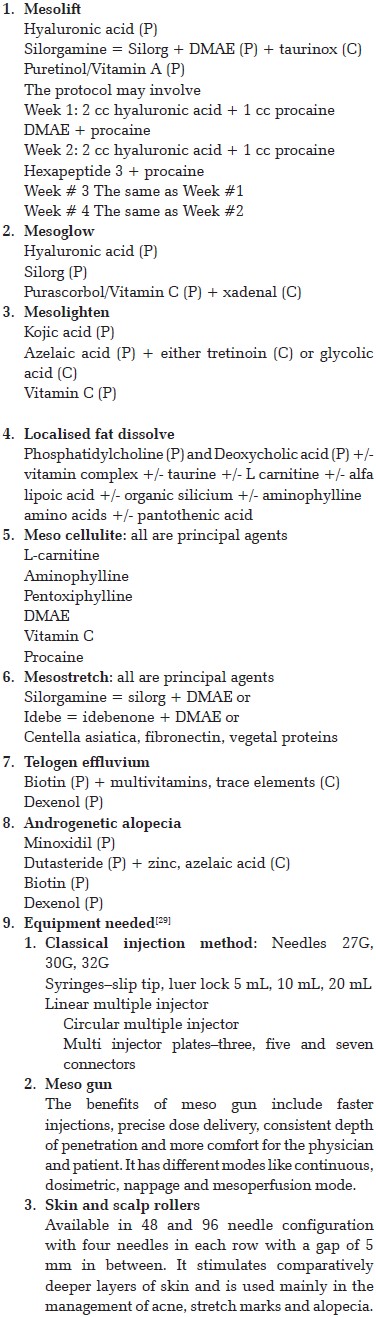
After obtaining informed consent, the physician will clean the skin of the patient with alcohol-free antiseptic solution and topical anesthetic can be used. Then, multiple injections are given with the needles mentioned above or mesogun is used [Figure - 1]. Each session takes about 10-30 min. In general, one to three sessions in acute cases, such as sports injuries, and 10-15 with maintenance sessions every 6 months or a year for chronic conditions such as "cellulite" may be required. There is no standardized formulation for mesotherapy and ingredients vary depending on indications. Commonly used techniques are: [4]
 |
| Figure 1: Mesogun |
Point by point
It involves injection of 0.02-0.05 mL of drug solution perpendicular to the skin (4 mm deep), about 1-2 cm apart. Mainly used for fat reduction.
Nappage (French for "covering")
It involves more superficial (2 mm deep) injections, given at a 45 degree angle from the skin while applying light, constant positive pressure on the plunger. [4] At each site, a drop of solution is introduced. Relatively, this is a more discomforting procedure to the patient.
Epidermic
It is the most superficial (1 mm deep) of all the techniques in which the basal layer of the skin is not penetrated. The needle is introduced and dragged along with light, positive pressure applied to the plunger. [4] It is done in a grid pattern at 1-cm intervals over the entire affected area.
Papule forming
It involves injection of the drugs at the dermoepidermal junction, between 2 mm and 4 mm, raising a small papule. Mainly used for wrinkles, alopecia and mesobotox.
Mesoperfusion
Some experts use a special technique called "mesoperfusion," wherein the same volume is injected over 10 min instead of 30 s as in a normal session.
Methods to Improve Patient Satisfaction
- Individuals who are receiving mesotherapy should be informed beforehand that development of itching, bruising, soreness, burning sensation and swelling at the site of injection are normal and shows that the drug is working.
- Procedure should be briefly explained to the patient.
- Proper counselling should be given regarding the results of procedure prior to the procedure so that the patient will not expect complete cure.
- Local application of ice packs before and after the procedure increases the numbness and decreases the post-procedure swelling.
- Using local anesthetic is not mandatory, but makes the procedure more comfortable. To reduce the burning sensation, topical lidocaine 1 h before the procedure can be used.
- Loose clothing after the procedure.
- Massaging the treated site in between the sessions decreases the formation of nodules.
No Needle Mesotherapy
It is a new modification of mesotherapy by which both ionised and neutral drugs can be transported into the dermis and subcutaneous tissue. [30],[31] In this technique, the selected site is first pre-treated with dual wavelength laser light and then has four components:
- Electroporation: electric waves of three different frequencies creating electropores of about 40-250 microns on the skin. Then, the desired substances are made to pass through these pores by electro repulsion. [30],[31] However, neutral substances also can pass through the pores due to their shape.
- Active current: improves the vascularity and thus ensures that sufficient amount of product reaches the site.
- Hydrophoresis: water-soluble substances penetrate inside the skin.
- Cryophoresis: cold temperature locks the substances in the skin cells. [30],[31]
No needle mesotherapy (NNM) is used mainly in the treatment of cellulite, also for skin rejuvenation, hyperpigmentation of photo aging, reduction of wrinkles, pores and skin lifting tightening. [30],[31] Advantages of NNM when compared with mesotherapy are (a) it is completely painless, (b) no bruising, erythema, swelling, (c) materials can penetrate to deeper levels, (d) immediate/rapid response and (d) cost effective.
Contraindications of Mesotherapy
- PC-no specific contraindications, to be used in caution with antiphospholipid antibody syndrome. [28]
- Aminophylline-history of hypersensitivity to the drug, active peptic ulcer, seizure disorder.
- L carnitine-to be used with caution in patients with seizure disorder.
- Hyaluronic acid-known hypersensitivity to the drug, use of other quaternary ammonium compounds (as they precipitate HA).
- Pentoxiphylline, aminophylline-recent cerebral, retinal hemorrhage.
- Mannitol-renal disease, pulmonary edema.
- Caffeine-hypotension, ventricular tachycardia, anxiety, gastrointestinal side-effects.
- General-age <18 years, diabetes mellitus, body mass index >30, pregnancy, lactation.
- Severe cardiac, renal disease, thromboembolic phenomenon.
Legal Issues Related to Mesotherapy
- Usage of off-label drugs like aminophylline, procaine and isoproterenol unprofessionally and carelessness in mesotherapy, which can subject the physicians to negligence is a burning issue. Doctors can protect themselves by taking an informed consent and by discussing the off-label uses of the drugs with the patient.
- It is also seen that few physicians give alcohol to patients prior to mesotherapy for its sedative effect, which comes under negligence or medical malpractise on the part of the doctor.
Complications
Local
In contrast to the claims of mesotherapy being a safe, minimally invasive procedure, several side-effects have been reported. Non-specific adverse effects include nausea, vomiting, mild pain, skin hyperesthesia, edema, itching and erythema. [6],[7],[28]
Due to faulty technique: atypical mycobacterial infections (Mycobacterium fortuitum), ulcers and scarring, nodularity and irregularity. Other side-effects include atrophy, lipodystrophy, subcutaneous oleomas [32] (due to mineral oil or sesame seed oil injections per se or use of oil even as a vehicle for vitamin B12 or phosphatidyl choline) lichenoid eruption, post-inflammatory hyperpigmentation [6],[7],[28],[33] and rare complications like koebnerization in psoriasis, localized urticaria pigmentosa, granuloma annulare, non-infectious granulomatous panniculitis and Mycobacterium abscessus[34] infection. Treatment options for complications are limited. For mesotherapy-induced panniculitis, one of the potential effects of this procedure, dapsone may be effective. Topical and oral steroids and colchicine have been tried with some success in the treatment of oleoma. [32] However, complete surgical excision remains the treatment of choice to prevent recurrence.
Systemic
Hypersensitivity reactions, infections like HIV, hepatitis and, most importantly, non-tuberculous mycobacterium (Mycobacterium immunogenum), rise in liver enzymes with or without liver toxicity and demyelination of nerves due to large doses of phosphatidylcholine. [6],[7],[28] Ischemic colitis occurred in patients who were receiving mesotherapy and anti-obesity medications due to the combined vasoconstriction effect. [35]
Conclusion
In recent years, mesotherapy gained popularity due to its non-invasive, painless nature, but, till date, the mode of action of many products used in mesotherapy is either doubtful or unknown and there are no clear cut guidelines on the dosage and efficacy of the products. Also, there is insufficient data evaluating the safety of the technique and the medicines used. Thus, the use of this technique is debatable.
In spite of this, many new substances like platelet-rich plasma, peptides, growth factors and collagen are finding their way to enter the field of mesotherapy. Many new indications and new modifications like no needle mesotherapy are also on the rise.
To conclude, "We must be cautious about rejecting new ideas. Just as absence of proof is not proof of absence, lack of scientific validation is not proof that it does not work." [36] Thus, continued research and well-designed controlled scientific studies are required to substantiate the claims of effectiveness of these new products and techniques and to formulate guidelines and recommendations regarding their use for aesthetic applications.
| 1. |
Raghvendra, Tyagi S, Yadav P, Saxena S, Dodia RA, Patel TD. Mesotherapy- A non surgical cosmetic medicine treatment: A review. Int J Pharm Sci Rev Res 2010;4:45-7.
[Google Scholar]
|
| 2. |
Sivagnanam G. Mesotherapy- The French connection. J Pharmacol Pharmacother 2010;1:4-8.
[Google Scholar]
|
| 3. |
Herreros FO, Moraes AM, Velho PE. Mesotherapy: A bibliographic review. An Bras Dermatol 2011;86:96-101.
[Google Scholar]
|
| 4. |
Pistor M. What is mesotherapy? Chir Dent Fr 1976;46:59-60.
[Google Scholar]
|
| 5. |
Gillette, Bill. Mesotherapy: Valuable, versatile treatment option. Dermatol Times 2006 Jan; Sect. cosmetic Dermatology. 54-61.
[Google Scholar]
|
| 6. |
Sarkar R, Garg VK, Mysore V. Position paper on mesotherapy. Indian J Dermatol Venereol Leprol 2011;77:232-7.
[Google Scholar]
|
| 7. |
Vedamurthy M. Mesotherapy. Indian J Dermatol Venereol Leprol 2007;73:60-2.
[Google Scholar]
|
| 8. |
Marrif HI. Thyroid hormones and mesotherapy. Front Endocrinol (Lausanne) 2011;2:5.
[Google Scholar]
|
| 9. |
Rotunda AM, Suzuki H, Moy RL, Kolodney MS. Detergent effects of sodium deoxycholate are a major feature of an injectable phosphatidylcholine formulation used for localized fat dissolution. Dermatol Surg 2004;30:1001-8.
[Google Scholar]
|
| 10. |
Matarasso A, Pfeifer TM. Mesotherapy for body contouring. Plast Reconstr Surg 2005;115:1420-4.
[Google Scholar]
|
| 11. |
Rose PT, Morgan M. Histological changes associated with mesotherapy for fat dissolution. J Cosmet Laser Ther 2005;7:17-9.
[Google Scholar]
|
| 12. |
Park SH, Kim DW, Lee MA, Yoo Sc, Rhee SC, Koo SH, et al. Effectiveness of mesotherapy on body contouring. Plast Reconstr Surg 2008;121:179e-85e.
[Google Scholar]
|
| 13. |
Frisari P, Pinto R. Mesoglow and Mesolift to rejuvenate facial skin. Am J Mesotherapy Vol 5. Available from:http://mesotherapyworldwide.com/images/pdf/Vol_5_75_MESOLIFT.pdf. [Last accessed on 2012 Sep 25].
[Google Scholar]
|
| 14. |
Greco JF. Advantages of utilising freeze dried collagen sheets in non-surgical "Mesolift" of the neck and face. Am J Mesotherapy Vol. 6. Available from: http://www.mesotherapyworldwide.com/images/pdf/Vol_6_99_Collagen_MesoLift.pdf. [Last accessed on 2012 Sep 25].
[Google Scholar]
|
| 15. |
Lacarrubba F, Tedeschi A, Nardone B, Micali G. Mesotherapy for skin rejuvenation: Assessment of the subepidermal low-echogenic band by ultrasound evaluation with cross-sectional B-mode scanning. Dermatol Ther 2008;21(Suppl 3):S1-5.
[Google Scholar]
|
| 16. |
El-Domyati M, El-Ammawi TS, Moawad O, El-Fakahany H, Medhat W, Mahoney MG, et al. Efficacy of mesotherapy in facial rejuvenation: A histological and immunohistochemical evaluation. Int J Dermatol 2012;51:913-9.
[Google Scholar]
|
| 17. |
Hertzog B. The Mesobotox, a different concept from the injection of the botulinum toxin. Available from: http://www.estheticmeso.com/en/aesthetics-care/28-le-mesobotox-article-scientifique.html [Last accessed on 2012 Sep 25].
[Google Scholar]
|
| 18. |
Moftah N, Moftah N, Abd-Elaziz G, Ahmed N, Hamed Y, Ghannam B, et al. Mesotherapy using dutasteride-containing preparation in treatment of female pattern hair loss: Photographic, morphometric and ultrastructural evaluation. J Eur Acad Dermatol Venereol 2012 [In Press].
[Google Scholar]
|
| 19. |
Mysore V. Mesotherapy in management of hairloss-Is it of Any Use? Int J Trichol 2010;2:45-6.
[Google Scholar]
|
| 20. |
Duque-Estrada B, Vincenzi C, Misciali C, Tosti A. Alopecia secondary to mesotherapy. J Am Acad Dermatol 2009;61:707-9.
[Google Scholar]
|
| 21. |
Kadry R, Hamadah I, Al-Issa A, Field L, Alrabiah F. Multifocal scalp abscess with sub-cutaneous fat necrosis and scarring alopecia as a complication of scalp mesotherapy. J Drugs Dermatol 2008;7:72-3.
[Google Scholar]
|
| 22. |
Kashani MN, Sadr B, Nilforoushzadeh MA, Arasteh M, Babakoohi S, Firooz A. Treatment of acute cutaneous leishmaniasis with intralesional injection of meglumine antimoniat: Comparison of conventional technique with mesotherapy gun. Int J Dermatol 2010;49:1034-7.
[Google Scholar]
|
| 23. |
Kim DH, Je YJ, Kim CD, Lee YH, Seo YJ, Lee JH, et al. Can Platelet-rich Plasma Be used for skin rejuvenation? Evaluation of effects of platelet-rich plasma on human dermal fibroblast. Ann Dermatol 2011;23:424-31.
[Google Scholar]
|
| 24. |
PRP Mesotherapycells. Available from: http://www.arsmedical.info/template-features/ prp-mesotherapy.html. [Last accessed on 2012 Sep 25].
[Google Scholar]
|
| 25. |
Biomimetic Mesotherapy-Nanopeptides in Medicine. Available from: http://dermagenica.co.uk/wp-content/uploads/2012/07/booklet.pdf. [Last accessed on 2012 Sep 25].
[Google Scholar]
|
| 26. |
Hair treatment with autologous stem cells. Available from: http://www.arsmedical.info/template-features/autologus-stem-cells.html. [Last accessed on 2012 Sep 25].
[Google Scholar]
|
| 27. |
Growth factors mesotherapy. Available from: http://www.arsmedical.info/template-features/growth-factor-mesotherapy.html. [Last accessed on 2012 Sep 25].
[Google Scholar]
|
| 28. |
Adilson H. Mesotherapy Materia Medica. Am J Mesotherapy Sect Pharm 16-23. Available from: http://www.mesotherapyworldwide.com/images/pdf/Vol_6_100_Mesotherapy_Materia_Medica_web.pdf. [Last accessed on 2012 Sep 25].
[Google Scholar]
|
| 29. |
Mesotherapy worldwide catalogue 2010:1-8. Available from: http://www.mesotherapyworldwide.com/images/pdf/MESOTHERAPY%20WORLDWIDE%20PRODUCT.pdf. [Last accessed on 2012 Sep 25].
[Google Scholar]
|
| 30. |
Schied G. A different kind of Mesotherapy. Available from: http://www.mesotherapyworldwide.com/images/pdf/Vol_1_13_KIND.pdf. [Last accessed on 2012 Sep 25].
[Google Scholar]
|
| 31. |
Amitrano C, Cappelletti R, Torre R. New trends in Drug Delivery Systems: Mesoporation, a novel technique. Am J Mesotherapy 24-25. Available from: http://www.mesotherapyworldwide.com/images/pdf/Vol_1_12_TRENDS.pdf. [Last accessed on 2012 Sep 25].
[Google Scholar]
|
| 32. |
Ramos-e-Silva M, Pereira AL, Ramos-e-Silva S, Oleoma PJ. Rare complication of mesotherapy for cellulite. Int J Dermatol 2012;51:162-7.
[Google Scholar]
|
| 33. |
Outbreak of mesotherapy-associated skin reactions-District of Columbia area, Jan-Feb 2005. MMWR Morb Mortal Wkly Rep 2005;54:1127-30.
[Google Scholar]
|
| 34. |
Wongkitisophon P, Rattanakaemakorn P, Tanrattanakorn S, Vachiramon V. Cutaneous Mycobacterium abscessus Infection Associated with Mesotherapy Injection. Case Rep Dermatol 2011;3:37-41.
[Google Scholar]
|
| 35. |
Kim JB, Moon W, Park SJ, Park MI, Kim KJ, Lee JN, et al. Ischemic colitis after mesotherapy combined with anti-obesity medications. World J Gastroenterol 2010;16:1537-40.
[Google Scholar]
|
| 36. |
Atiyeh BS, Ibrahim AE, Dibo SA. Cosmetic mesotherapy: Between scientific evidence, science fiction, and lucrative business. Aesth Plast Surg 2008;32:842-9.
[Google Scholar]
|
Fulltext Views
34,982
PDF downloads
4,633





![[Table - 1]](#tbl_ijdvl_2013_79_1_127_104689_t1.jpg){kind=link}
![[Figure - 1]](#fig_ijdvl_2013_79_1_127_104689_f2.jpg){kind=link}