
Translate this page into:
Modified buried continuous vertical mattress suture: A novel technique for closure of long wounds under tension
Corresponding author: Prof. Somesh Gupta, Department of Dermatology and Venereology, All India Institute of Medical Sciences, New Delhi, India. someshgupta@aiims.edu
-
Received: ,
Accepted: ,
How to cite this article: Ahuja R, Najeeb A, Gupta S. Modified buried continuous vertical mattress suture: A novel technique for closure of long wounds under tension. Indian J Dermatol Venereol Leprol. 2024;90:814-6. doi: 10.25259/IJDVL_701_2023
Dear Editor,
The vertical mattress suture is a useful technique for closing wounds under tension and achieving wound margin eversion, but may lead to track-marks.1 Closure is done using non-absorbable sutures, which have to be removed later. Placing subcuticular sutures in such wounds under tension may cause wound dehiscence. We propose a continuous, knot-free, buried vertical mattress suture that achieves a tension-free closure with good eversion and also prevents track-marks.
This wound closure technique was employed on two patients. The first patient, a young girl with tuberous sclerosis, had a 4 cm × 1.5 cm fibrous cephalic plaque surgically removed from her forehead [Figure 1a]. The second patient, another young girl underwent the removal of a 4 cm × 0.5 cm naevus sebaceous located in the preauricular region [Figure 1b]. This novel wound closure technique yielded excellent aesthetic outcomes in both the patients [Figures 1c and 1d].

- Pre- and post-operative photographs using the modified buried continuous vertical mattress suture for skin closure. A large fibrous cephalic plaque on the forehead extending into the anterior hairline.

- Two weeks after excision of fibrous cephalic plaque.

- A linear plaque of naevus sebaceous on the left preauricular area.

- The preauricular area 2 weeks’ post-removal of naevus sebaceous plaque.
Both patients underwent simple elliptical excisions (3:1 ratio) under aseptic precautions. After thorough undermining, the deeper closure was performed with interrupted sutures using a 4-0 vicryl with taper-point needle. Thereafter, we used a continuous buried vertical mattress suture to achieve superficial closure and approximate the epidermis. This technique followed two key principles: employing the far-far-near-near method of vertical mattress suturing and ensuring that the needle entered the skin at the exit point of the previous suture, effectively burying the stitch.
Using a 4-0 vicryl with a taper point needle, two angulated bites were taken beyond the wound edge to grasp tissue under the suture. The needle was then passed from the apex of the incision across to the far point on one side of the wound edge (far) [Figure 2a] and was then re-introduced at the previous exit point, advancing across to the far opposite end in a deeper plane (far-far) [Figure 2b]. Next, it was brought out at the near edge on the same side in a superficial plane (far-far-near) and then onto the near opposite edge (far-far-near-near) [Figure 2c]. Each insertion of the needle was done at the previous point of exit. The needle was subsequently passed from this near wound edge in a superficial plane onto the far contralateral edge in a deeper plane, about 0.5–1 cm from the previous VMS. [Figure 2d]. This process was repeated across the wound length. Finally, the suture was brought out beyond the opposite wound apex and secured in the tissue with consecutive angulated bites. Pulling both ends of the suture brought the two wound edges closer. The free ends of the suture were cut just at the surface, resulting in a completely buried suture without a knot, eliminating the need for removal [ Video 1].
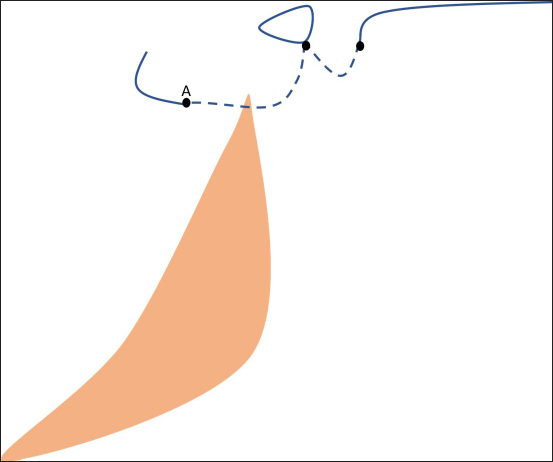
- Schematic diagram to demonstrate the steps in continuous buried vertical mattress suturing. Two consecutive bites are taken beyond the wound edge to get a hold of tissue under the suture. The needle is then advanced through the apex to the far end (point A) of one of the wound edges in a deeper plane (far).
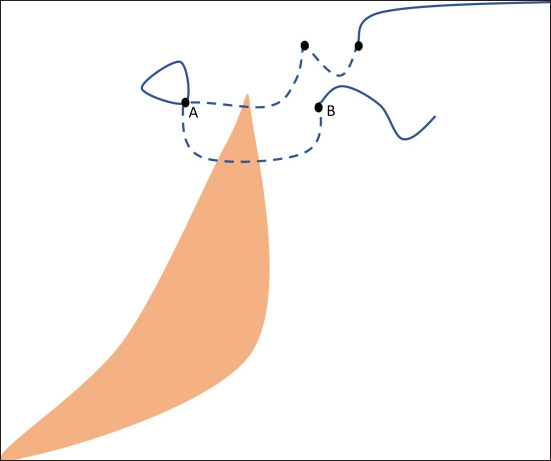
- The needle re-enters the skin through the same exit point (point A) to exit at the far opposite end (point B) in a deeper plane (far-far).
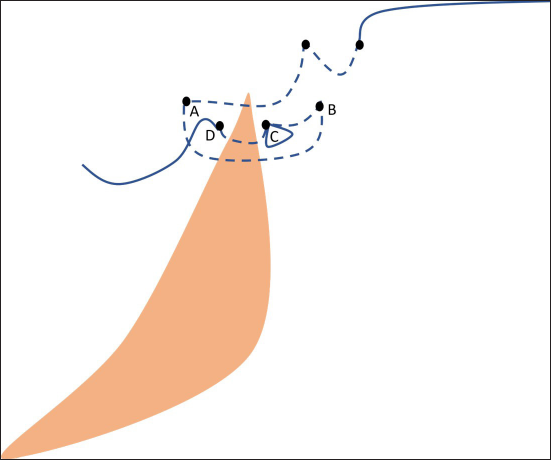
- After having passed through point A (far end), the needle re-enters at point B to exit at the near end on the same side (point C) and then re-enters through point C to exit at the near end on the opposite edge (point D) in a superficial plane (far-far-near-near).
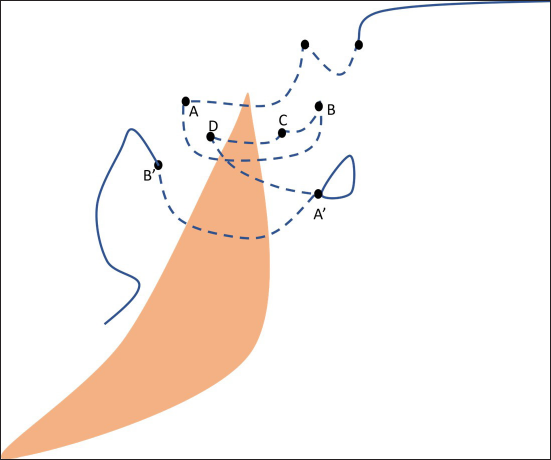
- After passing through points A, B and C, the needle re-enters the skin through point D and exits the far contralateral edge (point A’) in a deeper plane, about 1 cm from the previous vertical mattress. It again exits at the far opposite end (point B’) and the same process is followed through the length of the wound.
When performing this suture, especially for beginners, these key points should be kept in mind: first, always fully pull the suture through after each stitch to prevent poor wound approximation and gaping, as this is a continuous unlocked suture; and second, ensure you have enough suture material ready before starting, as you will not be cutting it at any point during the procedure.
At the two-week follow-up, the wounds showed optimal apposition, with minimal visibility of the needle entry marks. Moreover, there was no need for a non-absorbable suture for epidermal approximation, as the entire wound closure was performed using absorbable vicryl.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Reference
- The mattress sutures: vertical, horizontal, and corner stitch. Am Fam Physician. 2002;66:2231-6.
- [PubMed] [Google Scholar]




