Translate this page into:
Monthly rifampicin, ofloxacin, and minocycline therapy for generalized and localized granuloma annulare
Correspondence Address:
Shilpa Garg
22/11, Geeta Mandir Marg, New Rajinder Nagar, New Delhi - 110 060
India
| How to cite this article: Garg S, Baveja S. Monthly rifampicin, ofloxacin, and minocycline therapy for generalized and localized granuloma annulare. Indian J Dermatol Venereol Leprol 2015;81:35-39 |
Abstract
Background: The localized form of granuloma annulare is usually self-limiting, resolving within 2 years. Generalized granuloma annulare, on the other hand, runs a protracted course, with spontaneous resolution being rare. It is also characterized by a later age of onset, an increased incidence of diabetes mellitus, poor response to therapy, and an increased prevalence of HLA Bw35. Objective: To assess the efficacy of monthly pulsed rifampicin, ofloxacin, and minocycline (ROM) therapy in the management of granuloma annulare. Methods : Six biopsy proven patients of granuloma annulare were included in the study, five of the generalized variety, and one localized. Three of these patients were resistant to standard modalities of treatment. All six patients were treated with pulses of once monthly ROM till complete resolution of all lesions. Results were analyzed in terms of complete resolution of lesions and side effects. Presence of comorbid conditions was noted. Result: All six patients were successfully treated with 4-8 pulses of monthly ROM. None of the patients reported any adverse effects. Limitations: Small sample size and the lack of a control group are limitations. Conclusion: Treatment with pulses of once monthly ROM caused complete resolution of lesions in both localized and generalized granuloma annulare, even in cases recalcitrant to conventional therapy. There were no side effects in any of the patients. Larger trials are needed to substantiate the efficacy of monthly ROM in granuloma annulare.INTRODUCTION
Localized granuloma annulare is usually a self-limiting dermatosis resolving within 2 years. Generalized granuloma annulare which most frequently affects women older than 40 years, presents as multiple 1-2 mm skin colored papules involving the trunk, neck, forearms, legs, and extensor surface of elbows. It differs from the localized form by a later age of onset, protracted course with only rare spontaneous resolutions, an increased incidence of diabetes mellitus and a poor response to therapy. [1] An increased prevalence of HLA Bw35 has been seen in this form of the disease. [2] Treatment options for granuloma annulare include topical and systemic steroids, psoralen ultraviolet-A, isotretinoin, dapsone, pentoxifylline, hydroxychloroquine, cyclosporine, interferon gamma, chlorambucil, potassium iodide, nicotinamide, niacinamide, salicylates, chlorpropamide, thyroxine, dipyridamole, methyl aminolevulinate photodynamic therapy, fumaric esters, etanerept, infliximab, adalimumab, and efalizumab. [3] We report six cases of biopsy proven granuloma annulare who were treated with pulses of monthly rifampicin, ofloxacin, and minocycline (ROM) therapy.
Methods
A prospective study was carried out in the department of dermatology at Base Hospital, Delhi Cantt, India in which patients presenting with granuloma annulare (both generalized and localized form) from October 2011 to March 2013 were recruited. The study included both fresh cases as well as those not responding adequately to conventional modalities of treatment. Presence of comorbid conditions was noted. The diagnosis of granuloma annulare was confirmed histopathologically in all the patients, who were then treated with once monthly single dose of rifampicin 600 mg, ofloxacin 400 mg, and minocycline hydrochloride 100 mg till complete resolution of all lesions. Results were analyzed in terms of complete resolution of lesions and side effects. Patients were followed up for at least 6 months. Approval from ethical committee of our hospital was taken for the study.
Results
Between October 2011 and March 2013, a total of six patients with granuloma annulare were seen in the outpatient department, five with generalized and one with the localized form, all of whom were recruited to the study. The details of all the patients are mentioned in [Table - 1].
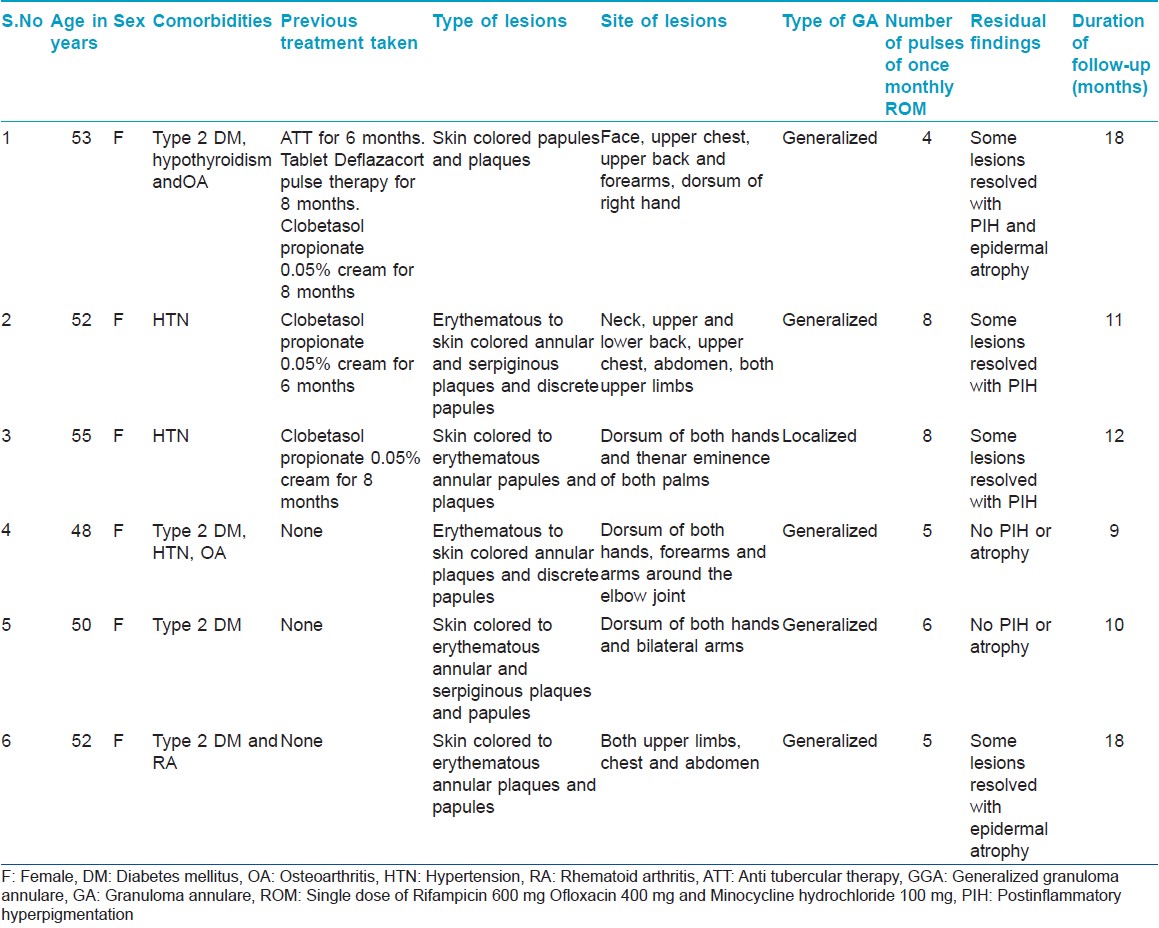
The diagnosis of granuloma annulare was confirmed histopathologically in all the patients. Special stains for mucin and acid fast bacilli were not done. Work-up did not reveal any evidence of malignancies or infection. All the patients responded well to ROM therapy with resolution of their lesions. Patients tolerated the treatment well with no side effects.
DISCUSSION
We had earlier [4] reported on the efficacy of ROM therapy in a single case of generalized granuloma annulare, with Type II diabetes mellitus and rheumatoid arthritis, who responded to five pulses of monthly ROM. [4] An extensive literature search threw up only one other study of monthly ROM used for this condition .[5] Marcus et al. reported six patients with granuloma annulare refractory to different kinds of treatment with hydrocortisone 1%, pimecrolimus, desoximetasone, mometasone furoate, clarithromycin, tacrolimus, fluticasone propionate, intralesional triamcinolone acetonide 40 mg/mL, liquid nitrogen, excimer laser, and topical triamcinolone 0.1%. The patients were treated with monthly ROM for 3 months. Three to five months after the initiation of treatment, the plaques cleared completely.
The rationale for using monthly ROM therapy for treating granuloma annulare is based on the clinical and histopathological similarities between this problem and paucibacillary leprosy, as well as their response to dapsone and prolonged antibiotic use. [6],[7],[8] Other antimicrobial agents have also been used for the treatment of granuloma annulare, postulating an infectious aetiology. [3]
Rifampicin has antimicrobial activity, and can influence antibody formation and cellular immune response, specifically delayed-type hypersensitivity. [6] Ofloxacin interferes with protein synthesis, inflammation, immunomodulation, cell proliferation, and angiogenesis, even in subantibiotic concentrations. [7] Minocycline reduces collagenase activity, interferes with lymphocyte proliferation, especially T cells, and has an anti-inflammatory effect. [8]
Our first patient [Figure - 1], a known case of type 2 diabetes mellitus, hypothyroidism, and osteoarthritis on regular treatment, presented with generalized granuloma annulare, which was confirmed histopathologically. Owing to the lack of response with prolonged oral steroid pulse therapy along with topical superpotent steroids, and the generalized nature of the lesions, she was treated with monthly ROM therapy for 4 months, to which she responded well, with complete clearance of lesions and without experiencing any side effects. Of special interest was her lack of response to antitubercular therapy, which entailed daily ingestion of rifampicin, in contrast to complete clearance of lesions with ROM pulses for 4 months. A possible explanation for this could be that only the combination (ROM) is efficacious, and not rifampicin alone.
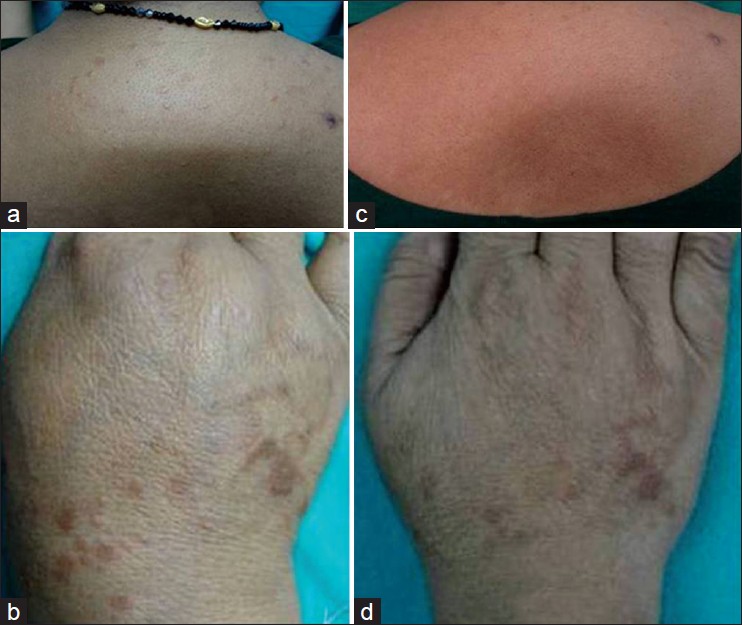 |
| Figure 1: (a) Discrete papular lesions of GGA involving the upper back (b) Hyperpigmented papules, plaques, and serpiginous lesions present on the dorsum of right hand (c) Complete resolution of lesions involving the upper back (d) Resolution of lesion on hand with PIH and atrophy |
Our second [Figure - 2] and third case [Figure - 3] had generalized and localized granuloma annulare respectively, and were recalcitrant to topical superpotent steroids but responded completely to 8 monthly pulses of ROM. The fourth [Figure - 4] and fifth case [Figure - 5] of generalized granuloma annulare, both of whom responded to 5-8 pulses of monthly ROM.
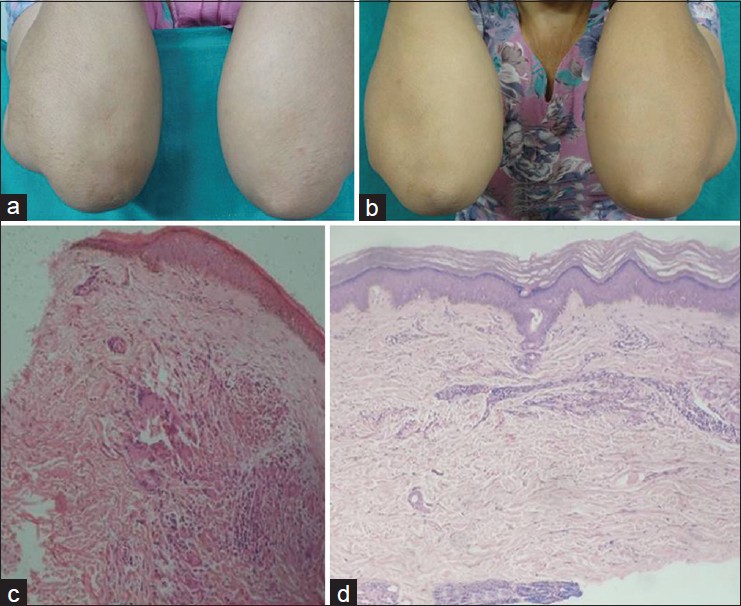 |
| Figure 2: (a) Discrete skin colored papule on the extensor surface of forearms (b) Resolution of lesions after ROM therapy (c) Granulomas with giant cells in the dermis (H and E, ×10) (d) Repeat histopathological examination after the resolution of lesion with monthly pulses of ROM therapy shows hyperkeratotic epidermis with sparse lympho-mononuclear cell infiltrate in the dermis Granulomas are absent (H and E, ×10) |
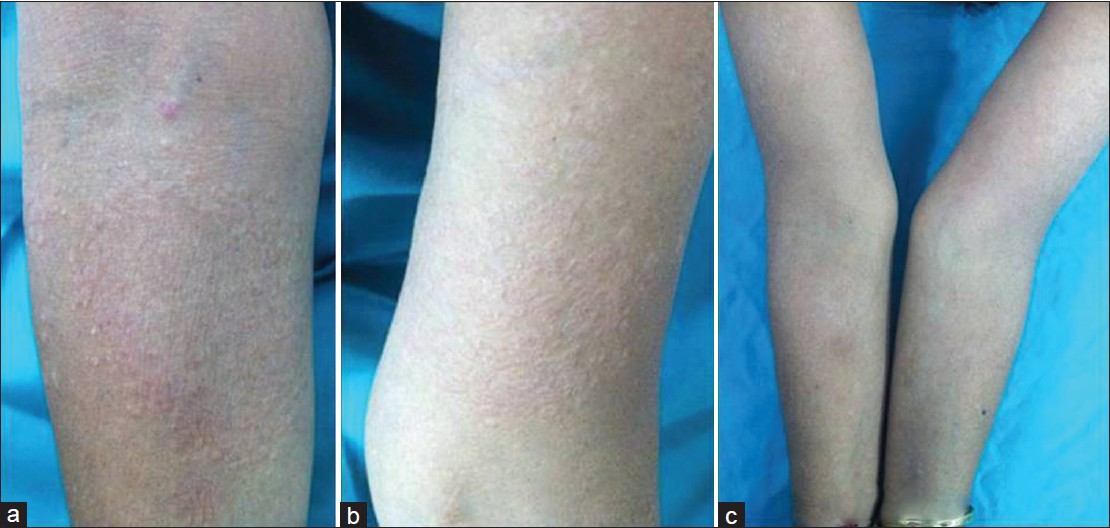 |
| Figure 3: (a) Multiple skin colored to erythematous papules coalescing to form an annular plaque on forearm (b) Multiple skin colored papules and plaques on arm (c) Resolution of lesions on forearm and arm |
 |
| Figure 4: (a) Multiple papules on dorsum of hand (b) Resolution of lesions with few lesions healing with atrophy |
 |
| Figure 5: (a) Annular plaques present on dorsum of both hands (b) Erythematous papules and serpiginous plaques on forearm and arm (c) Resolution of lesions on dorsum of hands after 6 monthly pulses of ROM (d) Resolution of lesions after 6 monthly pulses of ROM |
In this study, all the patients had complete clearance of lesions with a maximum of eight pulses of monthly ROM with no recurrence in the follow-up period. None of the drugs that the patients were taking for diabetes mellitus, hypertension, hypothyroidism, rheumatoid arthritis, or osteoarthritis was known to cause granuloma annulare.
Though granuloma annulare is known to resolve spontaneously, the generalized form usually runs a protracted course, with only rare spontaneous resolution. However, the consistency of response in all the six patients in this study, and a lack of recurrence during the follow-up period of 9-18 months seems to indicates a role of monthly ROM in the treatment of granuloma annulare.
The association of granuloma annulare with several comorbid conditions like Type 1 [9] and Type 2 diabetes mellitus, thyroid disease, malignancy, and dyslipidemias [10] has been observed. In our study also, all our patients had associated co-morbidities with three having more than one.
CONCLUSION
ROM pulses appears to be a highly effective, simple, non-invasive, less costly, and safe alternative in treating both forms of granuloma annulare. The association of multiple co-morbid conditions in all our patients reaffirms the need for a thorough screening for their detection. In view of the small sample size, ROM pulse therapy requires validation with studies involving larger numbers of patients.
| 1. |
Dicken CH, Carrington SG, Winkelmann RK. Genearalized granuloma annulare. Arch Dermatol 1969;99:556-63.
[Google Scholar]
|
| 2. |
Friedman-Birnbaum R, Haim S, Gigeone O, Barzilai A. Histocompatibility antigens in granuloma annulare: Comparative study of generalized and localized types. Br J Dermatol 1978;98:425-8.
[Google Scholar]
|
| 3. |
Shelley ED. Granuloma annulare. In: Shelley ED, Shelley WB, editors. Advanced dermatologic therapy. Vol 2. Philadelphia, PA: WB Saunders Ltd; 2001. p. 491-8.
[Google Scholar]
|
| 4. |
Garg S, Baveja S. Generalized granuloma annulare treated with monthly Rifampicin, Ofloxacin, and Minocycline combination therapy.Indian J Dermatol 2013;58:197-9.
[Google Scholar]
|
| 5. |
Marcus DV, Mahmoud BH, Hamzavi IH. Granuloma annular treated with rifampicin, ofloxacin, and minocycline combination therapy. Arch Dermatol 2009;145:787-9.
[Google Scholar]
|
| 6. |
Steiner A, Pehamberger H, Wolff K. Sulphone treatment of granuloma annulare. J Am Acad Dermatol 1985;13:1004-8.
[Google Scholar]
|
| 7. |
Villahermosa LG, Fajardo TT Jr, Abalos RM, Cellona RV, Balagon MV, Dela Cruz EC, et al. Parallel assessment of 24 monthly doses of rifampicin, ofloxicin, and minocycline versus two years of World Health Organization multi-drug therapy for multi-bacillary leprosy. Am J Trop Med Hyg 2004;70:197-200.
[Google Scholar]
|
| 8. |
Duarte AF, Mota A, Pereira MA, Baudrier T, Azevedo F. Generalized granuloma annulare-response to doxycycline. J Eur Acad Dermatol Venereol 2008;23:84-5.
[Google Scholar]
|
| 9. |
Maschio M, Marigliano M, Sabbion A, Morandi A, Schena D, Colato C, et al. A rare caseof granuloma annulare in a 5-year-old child with type 1 diabetes and autoimmune thyroiditis. Am J Dermatopathol2013;35:385-7.
[Google Scholar]
|
| 10. |
Thornsberry LA, English JC 3 rd . Etiology, diagnosis, and therapeutic management of granuloma annulare: An update. Am J Clin Dermatol2013;14:279-90.
[Google Scholar]
|
Fulltext Views
9,500
PDF downloads
2,882





![[Table - 1]](#tbl_ijdvl_2015_81_1_35_148564_t1.jpg){kind=link}
![[Figure - 1]](#fig_ijdvl_2015_81_1_35_148564_f2.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2015_81_1_35_148564_f3.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2015_81_1_35_148564_f4.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2015_81_1_35_148564_f5.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2015_81_1_35_148564_f6.jpg){kind=link}