
Translate this page into:
Multi drug failure of tinea corporis to terbinafine, itraconazole and fluconazole; translating extensive Indian microbiological and resistance data to a trial of ketoconazole with remarkable efficacy

Corresponding author: Dr. Kabir Sardana, Department of Dermatology, Atal Bihari Vajpayee Institute of Medical Sciences and Dr. Ram Manohar Lohia Hospital, Connaught Place, New Delhi, Delhi, India. kabirijdvl@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Sharath S, Sardana K, Khurana A. Multi drug failure of tinea corporis to terbinafine, itraconazole and fluconazole; translating extensive Indian microbiological and resistance data to a trial of ketoconazole with remarkable efficacy. Indian J Dermatol Venereol Leprol. doi: 10.25259/IJDVL_497_2024
Dear Editor,
The emergence of recalcitrant dermatophytosis caused by Trichophyton indotineae species has led to significant alterations in the clinical presentation and drug resistance patterns, posing difficulties in the treatment with inadequate response to first-line antifungal drugs, particularly terbinafine (TRB).
A 39-year-old woman presented with tinea corporis et cruris et faciei [Figure 1] for eight months. She had failed to respond to multiple topical and oral medications, including conventional itraconazole (ITZ) 100 mg twice daily (eight weeks), super bioavailable ITZ (SUBA-ITZ) 130 mg once daily (12 weeks), fluconazole 50 mg once daily (four weeks), TRB 250 mg twice daily (eight weeks) and topical clotrimazole, sertaconazole and luliconazole. Potassium hydroxide mount of skin scrapings revealed thin branching septate hyphae [Figure 2]. DNA sequencing of the 28S rRNA gene (internal transcribed spacer) identified the isolate as Trichophyton mentagrophytes/T. interdigitale species complex and antifungal susceptibility testing using micro titre broth dilution method revealed that as compared to the standard strain (T. mentagrophytes MTCC7687), the clinical isolate was less susceptible (minimal inhibitory concentration [MIC] 50 µg/mL) to fluconazole (16) and terbinafine (8), but was susceptible to ketoconazole (0.25), itraconazole (0.06) and luliconazole (0.03).

- Scaly plaques suggestive of tinea corporis on the gluteal area.
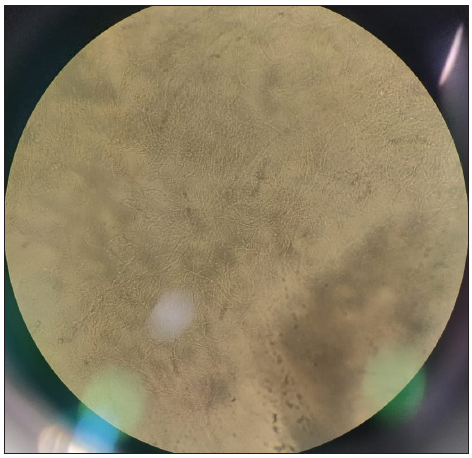
- Multiple thin branching septate hyphae (potassium hydroxide mount from skin scrapings, 400x).
In view of the clinical failure to other first-line systemic antifungals, she was administered oral ketoconazole 200 mg twice daily (with regular monitoring of liver function tests) and ciclopirox olamine 1% cream twice daily and responded to this regimen within four weeks with complete clearance of lesions [Figure 3] and a negative potassium hydroxide smear examination. Ketoconazole was continued for six weeks and stopped. No side effects were noted. She continues to be under follow-up without relapse for the past eight months.

- Complete resolution of lesions leaving behind post-inflammatory hyperpigmentation after four weeks of treatment with ketoconazole 200 mg twice daily and ciclopirox cream 1% cream twice daily.
Unlike controlled trials where drugs are compared with a placebo, real-world experience is markedly different and is exemplified in our scenario not encountered in the published data emanating from the Western countries. Treatment of dermatophytosis has become difficult and prolonged since the emergence of the novel species – T. indotineae. Previous data has shown consistently higher MICs to terbinafine (4 to >32 µg/mL),1 leading to reduction in its clinical efficacy. Also, MICs of fluconazole and griseofulvin have been consistently high with consequent clinical failures.2 While itraconazole has had consistently low MICs (MIC90–0.5 µg/mL),3 the quality of pellet-based conventional ITZ formulations is an important consideration4 for clinical failure. Our patient was however administered SUBA-ITZ which obviates the issue of pellet variability.
Failure of itraconazole in such a scenario suggests mutations in efflux pumps, which has been recently published from India.5 Notably, generating data on resistance mechanism is expensive and time consuming6 and it is incumbent to rely on country specific data to treat patients of dermatophytosis. We thus translated the synergy data of an Indian study3 and administered ketoconazole7 as a last option with remarkable results and long-term remission.
Ketoconazole acts by inhibiting the synthesis of ergosterol in the fungal cell wall and demonstrates higher keratin adherence. While ketoconazole usage is limited due to reports of hepatotoxic potential, a recent study highlighted the safety of ketoconazole with only transient elevation in liver enzymes in 4% patients which subsided post discontinuation of the drug.7
Thus, ketoconazole may be used as a last option drug in cases with multidrug failures, a scenario being increasingly encountered with an uptick of T. indotineae and can be considered in view of the prevalent Indian data on MIC1,3,5,6 and lack of hepatotoxicity which is a perceived concern with the drug.7
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Correlation of in vitro susceptibility based on MICs and squalene epoxidase mutations with clinical response to terbinafine in patients with tinea corporis/cruris. Antimicrob Agents Chemother. 2018;62:e01038-18.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- The science and rationale of arriving at the correct drug and dosimetry of griseofulvin, fluconazole, terbinafine and itraconazole in superficial dermatophyte infections: An important step before a pragmatic trial. Br J Dermatol. 2021;184:376-77.
- [CrossRef] [PubMed] [Google Scholar]
- Checkerboard analysis to evaluate synergistic combinations of existing antifungal drugs and propylene glycol monocaprylate in isolates from recalcitrant tinea corporis and cruris patients harboring squalene epoxidase gene mutation. Antimicrob Agents Chemother. 2021;65:e0032121.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- An exploratory pilot analysis of the optimal pellet number in 100 mg of itraconazole capsule to maximize the surface area to satisfy the noyes-whitney equation. J Dermatolog Treat. 2021;32:788-94.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment recalcitrant cases of tinea corporis/cruris caused by T. mentagrophytes – interdigitale complex with mutations in ERG11 ERG 3, ERG4, MDR1 MFS genes & SQLE and their potential implications. Int J Dermatol. 2023;62:637-48.
- [CrossRef] [PubMed] [Google Scholar]
- An update on the myriad antifungal resistance mechanisms in dermatophytes and the place of experimental and existential therapeutic agents for Trichophyton complex implicated in tinea corporis and cruris. Expert Rev Anti Infect Ther. 2023;21:977-91.
- [CrossRef] [PubMed] [Google Scholar]
- Real world analysis of response rate and efficacy of oral ketoconazole in patients with recalcitrant tinea corporis and cruris. Am J Trop Med Hyg. 2021;106:38-44.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]




