Translate this page into:
Multifocal extra-ocular sebaceous carcinoma
2 Department of Pathology, St. John's Medical College Hospital, Bangalore-560 034, India
Correspondence Address:
Ishwara P Bhat
Department of Dermatology, St. John's Medical College Hospital, Bangalore-560 034
India
| How to cite this article: Bhat IP, Madhukara J, Elizabeth J, Kini U, Anuradha A. Multifocal extra-ocular sebaceous carcinoma. Indian J Dermatol Venereol Leprol 2011;77:403 |
Sir,
Sebaceous carcinomas are uncommon, aggressive, malignant neoplasms derived from the adnexal epithelium of sebaceous glands. Approximately 75% of these tumors arise in the periocular region, commonly arising from the Meibomian glands of the eyelid. [1] Extra-ocular sebaceous carcinomas are very uncommon and usually arise on the head and neck. [2]
A 32-year-old male presented with a history of gradually spreading papules and nodules over the left lower limb for two years. These lesions started over the ankle as a small papule, which enlarged in size along with the appearance of new lesions. The patient had received multiple courses of antibiotics without much benefit. The general condition of the patient was good with no history of weight loss, abdominal pain, and pulmonary or neurological symptoms. Systemic examination revealed no abnormalities. Cutaneous examination showed multiple yellowish and skin-colored papules and nodules of firm consistency. While some lesions showed umbilication, others were ulcerated with secondary bacterial infection. They were distributed over the dorsum of the left foot, anterolateral aspect of the left leg and lower aspect of the thigh [Figure - 1]. The left popliteal and inguinal lymph nodes were enlarged, mildly tender, firm in consistency, not matted and not fixed to the underlying tissue. Clinically, a differential diagnosis of multiple molluscum contagiosum, atypical mycobacterial infection and sporotrichosis was considered.
 |
| Figure 1: Ulcerated nodules and papules on the leg |
Potassium hydroxide preparation from the aspirate of the lesion did not reveal any fungal elements or molluscum bodies. Routine blood counts, chest X-Ray, liver function tests and renal function tests were within normal limits. HIV serology was negative. Gram′s stain done showed Gram-positive cocci, which on culture grew Staphylococcus aureus. Histology of the nodule showed the infiltrating but lobular neoplasm in the dermis composed of oval to spindle-shaped pleomorphic cells with vesicular nuclei and abundant eosinophilic cytoplasm which appeared vacuolated at foci [Figure - 2]. These cells were seen dissecting through collagen bundles. This histology with clinical features prompted a diagnosis of sebaceous carcinoma. This was confirmed by additional histochemical staining, which was positive for Epithelial Membrane Antigen (EMA) [Figure - 3] and CD 15, typical of sebaceous carcinoma. Fine needle aspiration cytology from the popliteal and inguinal lymph nodes showed metastases of cells with similar morphology.
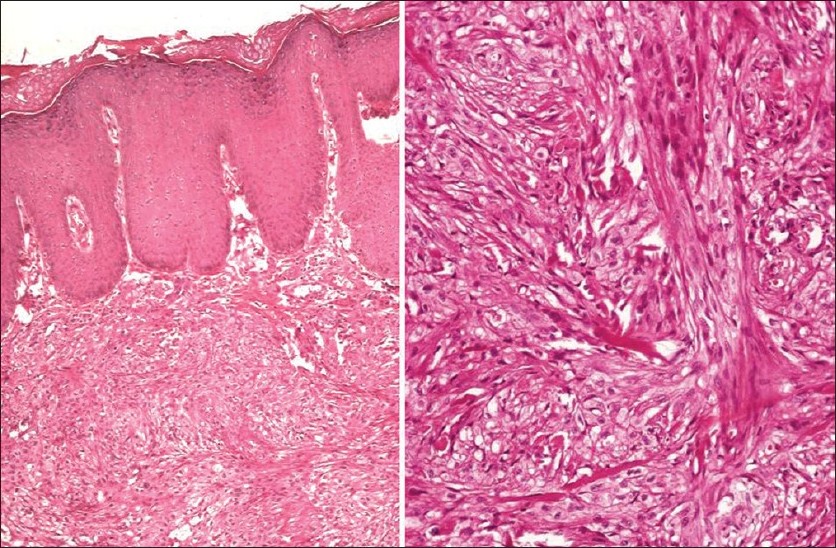 |
| Figure 2: Histopathology, hematoxylin and eosin stain showing pleomorphic malignant cells dissecting through collagen bundles ×400 |
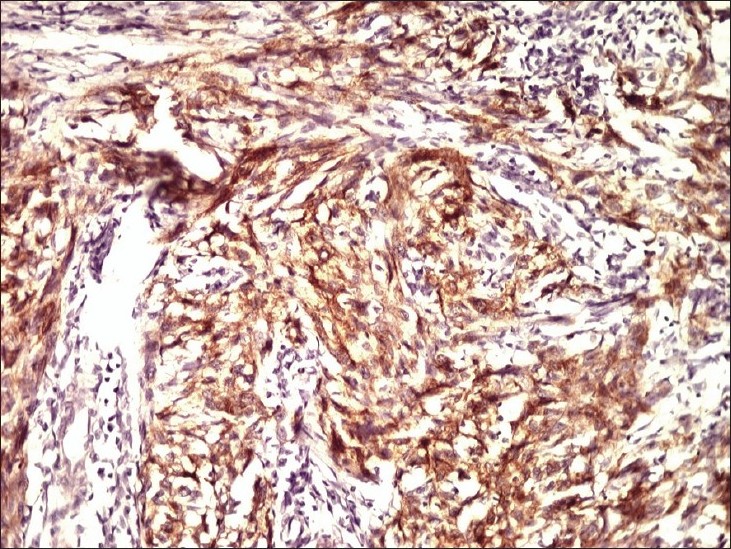 |
| Figure 3: EMA staining showing positive cells, ×400 |
A final diagnosis of primary multifocal sebaceous carcinoma with lymph node metastasis was made. Subsequently, detailed clinical reevaluation and relevant investigations (computed tomography scan, ultrasound) were carried out to rule out the Muir-Torre syndrome and distant metastases, which were negative. The patient was referred to the surgical oncologist for further management. He was advised amputation of the involved limb with subsequent chemotherapy.
Sebaceous carcinoma exhibits such a variety of histological growth patterns and diverse clinical presentations that the diagnosis is often delayed for months to years. It can clinically mimic benign conditions such as molluscum contagiosum, keratoacanthomas and benign adenexal tumors as seen with our case.
Extra-ocular sebaceous carcinomas are rare (< 25% of cases) and usually localize on the head and neck region. Primary lesions arising below the neck, as with our case, are extremely rare. They are aggressive and recurrent with a high mortality rate and have a strong association with visceral malignancies.
The Muir-Torre syndrome is an autosomal dominant condition with variable penetrance, and usually presents with benign and malignant sebaceous neoplasms, keratoacanthomas, and internal manifestations like tumors of the gastrointestinal and genitourinary tract [3],[4] In our case even though the Muir-Torre syndrome was considered, it was ruled out because of the absence of any features other than sebaceous carcinomas.
A varied histological appearance may occur. Histology reveals irregular lobular growth pattern composed of sebaceous and undifferentiated cells. [5] Solid/lobular growth patterns, bowenoid, pagetoid and comedocarcinoma-like patterns have been described. [5] Immunoperoxidase staining with EMA, BRST-1 (monoclonal antibody which detects BCA 225) and Cam 5.2 (anti cytokeratin monoclonal antibody) helps to distinguish sebaceous carcinoma from other neoplasms.
To the best of our knowledge, there are no reports of multifocal extra-ocular sebaceous carcinomas in the absence of the Muir-Torre syndrome or nevus sebaceous and probably, this is the first such case. Awareness of this condition is required among dermatologists to ensure early diagnosis of this highly aggressive neoplasm.
| 1. |
Akhtar S, Oza KK, Roulier RG. Multiple sebaceous adenomas and extraocular sebaceous carcinoma in a patient with multiple sclerosis: Case report and review of literature. J Cutan Med Surg 2001;5:490-5.
[Google Scholar]
|
| 2. |
Escalonilla P, Grilli R, Cañamero M, Soriano ML, Fariña MC, Manzarbeitia F, et al. Sebaceous carcinoma of the vulva. Am J Dermatopathol 1999;21:468-72.
[Google Scholar]
|
| 3. |
Prieto VG. Muir-Torre Syndrome. Emedicine. Available from: http://emedicine.medscape.com. [Last accessed on 2009 December 10].
[Google Scholar]
|
| 4. |
Entius MM, Keller JJ, Drillenburg P, Kuypers KC, Giardiello FM, Offerhaus GJ. Microsatellite Instability and Expression of hMLH-1 and hMSH-2 in Sebaceous Gland Carcinomas as Markers for Muir-Torre Syndrome. Clin Cancer Res 2000;6:1784-9.
[Google Scholar]
|
| 5. |
Pereira PR, Odashiro AN, Rodrigues-Reyes AA, Correa ZM, de Souza Filho JP, Burnier MN Jr. Histopathological review of sebaceous carcinoma of the eyelid. J Cutan Pathol 2005;32:496-501.
[Google Scholar]
|
Fulltext Views
2,119
PDF downloads
3,124





![[Figure - 1]](#fig_ijdvl_2011_77_3_403_79743_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2011_77_3_403_79743_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2011_77_3_403_79743_f3.jpg){kind=link}