Translate this page into:
Multiple asymptomatic papules on the glans penis
Correspondence Address:
Zhu Shen
Department of Dermatology, Southwest Hospital, Third Military Medical University, Chongqing 400038
China
| How to cite this article: Zhou C, Zhai Z, Yang X, Shen Z. Multiple asymptomatic papules on the glans penis. Indian J Dermatol Venereol Leprol 2015;81:431-433 |
A 71-year-old man presented with a 3-month history of asymptomatic glans penis lesions [Figure - 1] and [Figure - 2], with numerous red, indurated, partially fusing 1 mm papules. There was no inguinal lymphadenopathy. Complete blood count, routine urinalysis, stool microscopy and liver and renal function test results were normal. Results for a serological test for human immunodeficiency virus, and both the toluidine red unheated serum test (TRUST) and Treponema pallidum particle agglutination tests for syphilis were negative. The patient had been diagnosed with prostatic adenocarcinoma in May 2009. He had undergone surgery at that time and was receiving abiraterone acetate (Zytiga) treatment for the past 10 months. Computed tomography confirmed widespread osseous [Figure - 3] and lymphatic metastases; however, metastases were not observed in the retroperitoneal and pelvic lymph nodes at admission or 3 months later.
 |
| Figure 1: Multiple papules on the glans penis (dorsal side) |
 |
| Figure 2: Similar papules on the glans penis (ventral side) |
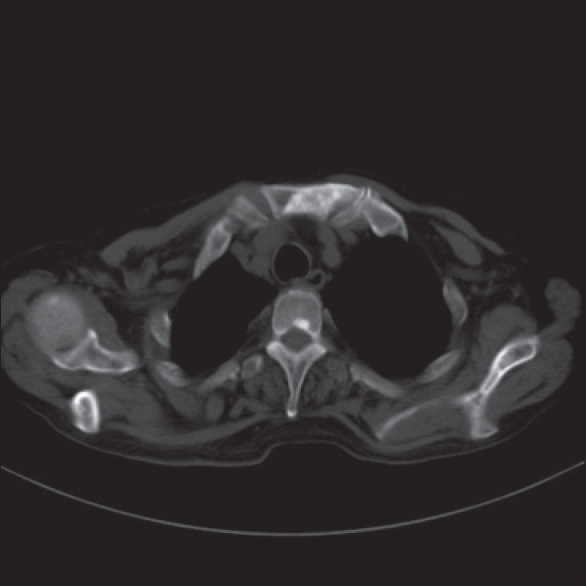 |
| Figure 3: Computed tomography scan showed metastasis of sternum, thoracic vertebra and spealbone |
Biopsy of the papule on the penis showed nests of poorly differentiated tumor cells in the whole dermis, with thinned epidermis [Figure - 4]. The tumor cells showed pale cytoplasm with gland formation [Figure - 5]. A few of the tumor cells were positive for prostate specific antigen (PSA) [Figure - 6]. The tumor cells were positive for cytokeratin [Figure - 7], but negative for P63, P504S, CD31, and D2-40.
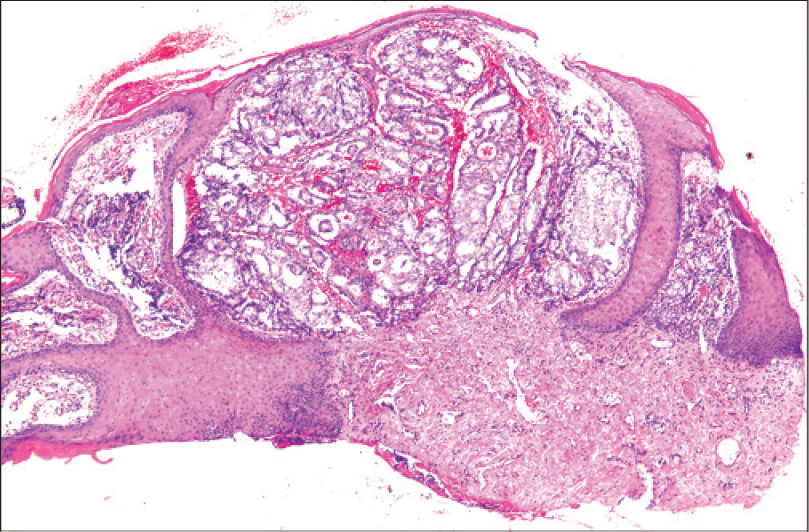 |
| Figure 4: A thinned epidermis and neoplastic cells filling the dermis (H and E, 25×) |
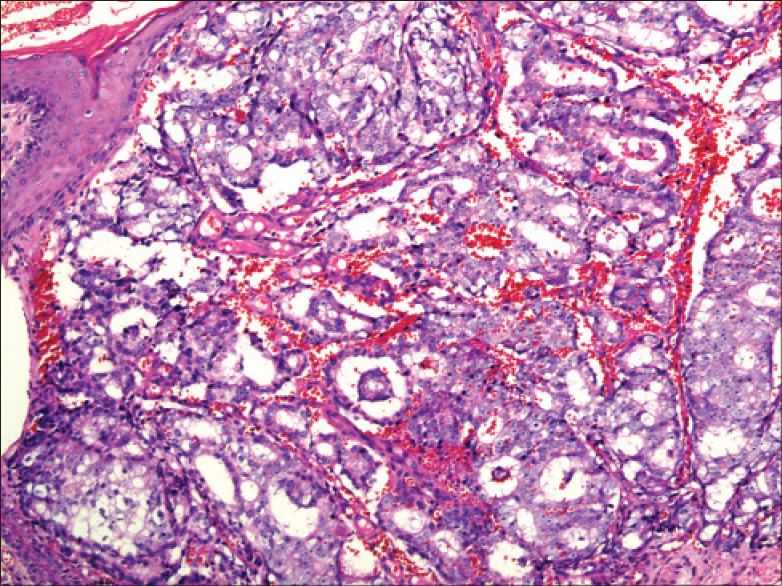 |
| Figure 5: The tumor cells with pale cytoplasm, showing adenoid formation (H and E, 100×) |
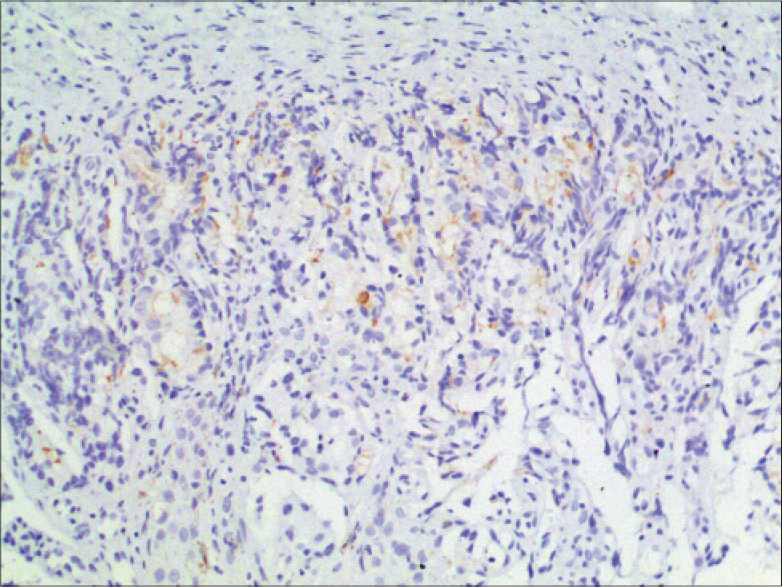 |
| Figure 6: Immunohistochemistry showing individual cytoplasmic positivity for prostate-specific antigen (200×) |
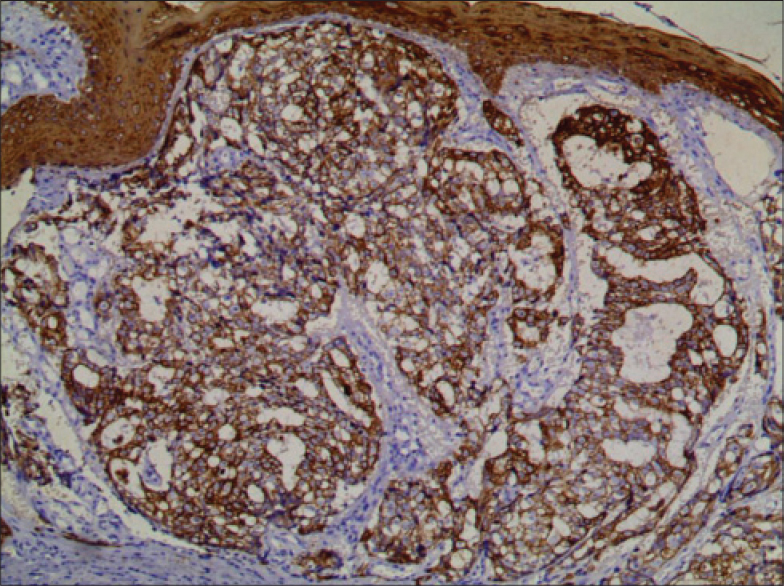 |
| Figure 7: Immunohistochemistry showing cytoplasmic positivity for cytokeratin (100×) |
What is your diagnosis?

| 1. |
Ansari H, Prashant R, Franks A. Prostatic carcinoma metastasis to the penis - an uncommon site. Lancet Oncol 2003;4:705-6.
[Google Scholar]
|
| 2. |
Gandaglia G, Abdollah F, Schiffmann J, Trudeau V, Shariat SF, Kim SP, et al. Distribution of metastatic sites in patients with prostate cancer: A population-based analysis. Prostate 2014; 74:210-6.
[Google Scholar]
|
| 3. |
Philip J, Mathew J. Penile metastasis of prostatic adenocarcinoma: Report of two cases and review of literature. World J Surg Oncol 2003;1:16.
[Google Scholar]
|
| 4. |
Kobashi-Katoh R, Tanioka M, Takahashi K, Miyachi Y. Skin metastasis of prostate adenocarcinoma to glans penis showing no correlation with serum prostate-specific antigen level. J Dermatol 2009;36:106-8.
[Google Scholar]
|
| 5. |
Kotake Y, Gohji K, Suzuki T, Watsuji T, Kusaka M, Takahara K et al. Metastases to the penis from carcinoma of the prostate. Int J Urol 2001;8:83-6.
[Google Scholar]
|
Fulltext Views
4,393
PDF downloads
3,377





![[Figure - 1]](#fig_ijdvl_2015_81_4_431_158661_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2015_81_4_431_158661_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2015_81_4_431_158661_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2015_81_4_431_158661_f4.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2015_81_4_431_158661_f5.jpg){kind=link}
![[Figure - 6]](#fig_ijdvl_2015_81_4_431_158661_f6.jpg){kind=link}
![[Figure - 7]](#fig_ijdvl_2015_81_4_431_158661_f7.jpg){kind=link}