Translate this page into:
Multiple dermatofibromas on face treated with carbon dioxide laser
Correspondence Address:
D S Krupa Shankar
Department of Dermatology, Manipal Hospital, 98, Rustom Bagh, Airport Road, Bangalore
India
| How to cite this article: Krupa Shankar D S, Kushalappa A A, Suma K S, Pai SA. Multiple dermatofibromas on face treated with carbon dioxide laser. Indian J Dermatol Venereol Leprol 2007;73:194-195 |
 |
| Figure 2: Multiple dermatofi bromas of the face before and after CO2 laser therapy |
|
| Figure 2: Multiple dermatofi bromas of the face before and after CO2 laser therapy |
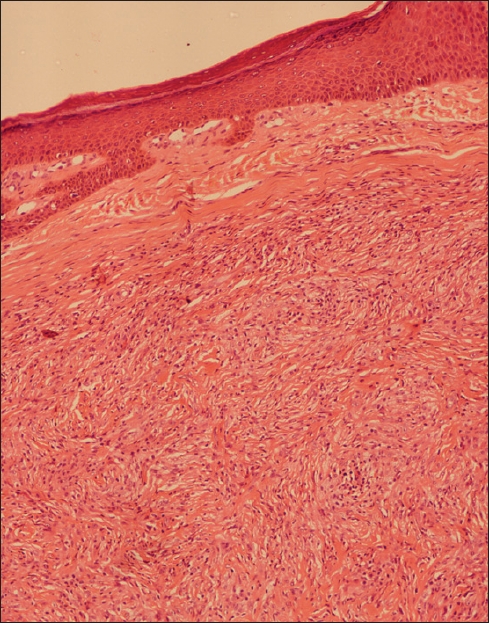 |
| Figure 1: A well circumscribed benign spindle cell lesion in the dermis (H and E, x100) |
|
| Figure 1: A well circumscribed benign spindle cell lesion in the dermis (H and E, x100) |
Sir,
Dermatofibroma is a benign tumor which is a generally a single round or ovoid papule or nodule about 0.5 mm to 1 cm in diameter, is reddish brown, sometimes with a yellowish hue. The commonest sites include thighs, legs or arms and affection of face is rare. We came across an unusual case of multiple dermatofibromas on the face and the trunk.
A 58-year-old man presented with skin-colored papules and nodules over the face, arms and trunk. He initially noticed one of them at the right outer angle of the eye. Lesions then appeared over the cheeks, eyelids, chin, neck, chest and arms. Gradually over a period of eight months, two lesions regressed spontaneously on the face. The patient had no history of medication for any illness. There was no relevant family or personal history.
Cutaneous examination revealed dry, firm to hard, round to oval, skin-colored nodules, ranging from one millimeter to two centimeters with regular borders. The lesions were scattered, regional and bilaterally symmetrical. The conjunctiva, mouth, scalp, hair and nails were normal. There were no cafι′ au lait macules. A clinical differential diagnosis of neurofibroma or xanthoma was considered.
One of the nodules on the face was excised with carbon dioxide laser and submitted for histopathological evaluation [Figure - 1]. A diagnosis of dermatofibroma was made. Subsequently, six lesions were excised using carbon dioxide laser with histology again showing features of dermatofibroma. Satisfactory healing was noted at one week and one month following excisions without significant scarring [Figure - 2]. The patient has been followed-up for eight months without any recurrences.
Dermatofibroma is characterized by a nodular cellular proliferation of fibroblasts in a criss-cross or storiform pattern in the dermis. Further, multinucleate giant cells and foam cells were also seen in our patient a feature that is common in dermatofibromas. Neurofibroma was ruled out as a possible diagnosis in the absence of cells with wavy nuclei or evidence of specific neurogenic differentiation. [1] Also retrospectively, a history of spontaneous remission of two lesions is consistent with a diagnosis of dermatofibroma. As simple excision was precluded given the number, size and location of the lesions, carbon dioxide laser was used to get a bloodless excision and wound contraction leading to a scar-free excision.
Dermatofibroma is believed to be a pattern of dermal response to injury such as insect bites. Whether its cell of origin is the fibroblast or histiocyte is still unclear. [2] One third of the lesions are multiple. [3] Multiple eruptive dermatofibromas have been reported, in patients with autoimmune diseases such as lupus erythematous and those on immunosuppressive drugs. [4],[5]
The course is benign with slow spontaneous involution. Less than 5% of dermatofibromas recur after excision. [6] Involution may occur after many years.
Carbon dioxide laser has benefits over other modalities in terms of absence or delay in recurrence due to influence on fibroblast secretion of growth factor. [7] In conclusion, we emphasize that dermatofibromas may clinically resemble neurofibromas or xanthomas, further multiple tumors can be effectively excised with carbon dioxide laser.
| 1. |
Halpryn IH, Allen AC. Epidermal changes associated with sclerosing haemangiomas. Arch Dermatol 1959;80:160.
[Google Scholar]
|
| 2. |
Bedi TR, Pandhi PK, Bhutani LK. Multiple palmoplantar histocytomas. Arch Dermatol 1976;122:1001-3.
[Google Scholar]
|
| 3. |
Gonzalez S, Duarte I. Benign fibrous histiocytoma of the skin. A morphologic study of 290 cases. Pathol Res Pract 1982;174:379-91.
[Google Scholar]
|
| 4. |
Kuniyuki S, Shindow K. Multiple dermatofibromas accompanied by eruptive benign keratosis in a patient with systemic lupus erythematosus. J Dermatol 1996;23:619-22.
[Google Scholar]
|
| 5. |
Toda S, Heasley DD, Carlson JA, Mihm MC Jr. Lentiginous melanocytic hyperplasia overlying dermatofibroma. J Dermatol 1996;23:840-4.
[Google Scholar]
|
| 6. |
Calonge E, Fletcher CD. Cutaneous fibrohistiocytic tumors: An update. Adv Anat Pathol 1994;1:2.
[Google Scholar]
|
| 7. |
Nowak KC, McCorack M, Koch RJ. The effect of superpulsed carbon dioxide laser energy on keloid and normal dermal fibroblast secretion of growth factors. Plast Reconstr Surg 2000;105:2039-48.
[Google Scholar]
|
Fulltext Views
5,472
PDF downloads
1,922





![[Figure - 1]](#fig_ijdvl_2007_73_3_194_32747_1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2007_73_3_194_32747_2.jpg){kind=link}