Translate this page into:
Multiple inflamed cutaneous nodules in an elderly female
Correspondence Address:
Kiran Preet Malhotra
Department of Pathology, Dr. Ram Manohar Lohia Institute of Medical Sciences, Gomti Nagar, Lucknow, Uttar Pradesh
India
| How to cite this article: Malhotra KP, Neyaz A, Gupta A, Das M, Husain N. Multiple inflamed cutaneous nodules in an elderly female. Indian J Dermatol Venereol Leprol 2018;84:518-520 |
A 65-year-old diabetic female presented with a discoloured, elevated lesion, approximately 5 cm in diameter, on her left thigh; which had been gradually increasing in size over the last month. She also complained of low-grade fever for the last 20 days. Recently, a similar lesion had also developed on her left lumbar region [Figure - 1]. She was treated with empirical antibiotics by the general physician as a case of multiple abscesses without any success. Her general condition also worsened with continuous fever and weight loss. An excision biopsy of the lesion and histopathological examination (HPE) revealed sheets of large pleomorphic cells infiltrating the epidermis, dermis and subcutaneous tissue. The cells possessed round to indented nuclei, occasional prominent nucleoli and pink cytoplasm. Necrosis and angioinvasion were noted [Figure - 2]. Other systemic examinations were within normal limits. Skin, hair and nails were spared. Peripheral blood smear was unremarkable. Amelanotic malignant melanoma, cutaneous lymphoma, metastatic carcinoma and epithelioid sarcoma were considered as differentials. The immunohistochemistry panel showed positivity for vimentin, leukocyte common antigen, CD3, CD56 and granzyme B in the tumor cells while Homatropine methylbromide-45, pan-cytokeratin, CD20, CD4, CD8 and CD30 were found to be negative [Figure - 3].
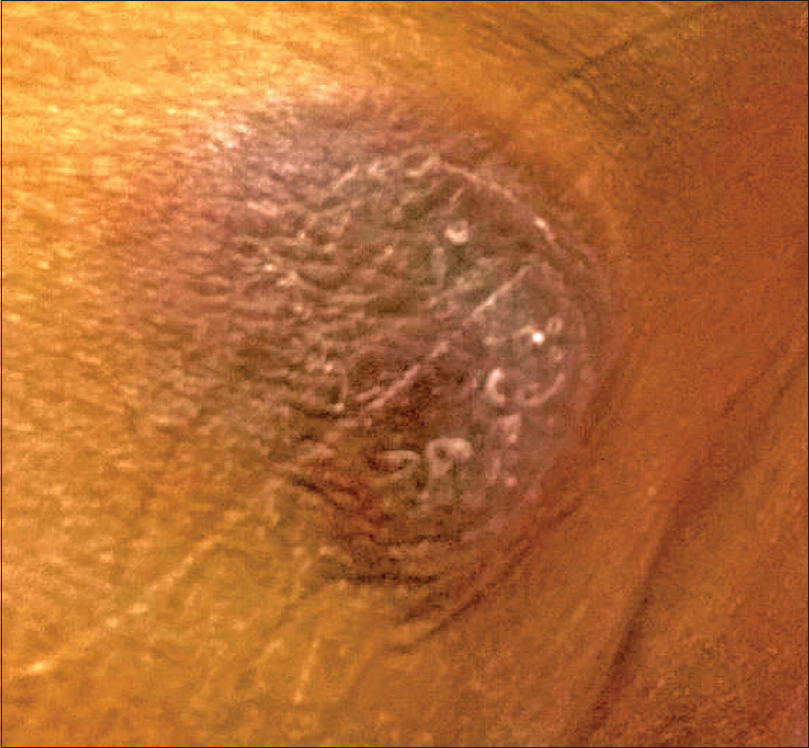 |
| Figure 1: Large abscess-like lesion on the left lumbar area |
 |
| Figure 2: (a) Section from skin shows epidermal and dermal infiltrate of lymphocytes demonstrating mild atypia (H and E, ×50) (b)Section shows sheets of cells with a focus of necrosis (left half of field) (H and E, ×100) (c) Section shows large cells with hyperchromatic pleomorphic nuclei and mitoses (arrows) (H and E, ×400) (d) Section shows a vessel with angioinvasion (H and E, ×400) |
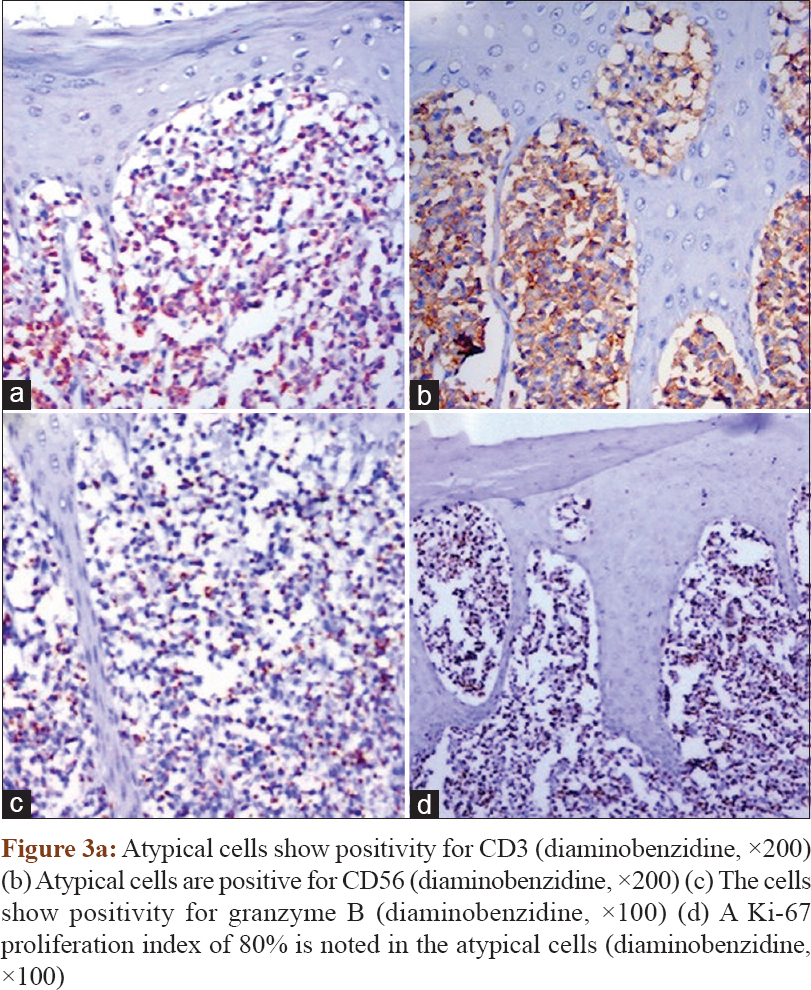 |
| Figure 3 |
What Is Your Diagnosis?
Answer
Extranodal natural killer T-cell lymphoma nasal type.
Discussion
Extranodal natural killer T-cell lymphoma nasal type is an Epstein–Barr virus-associated lymphoma that generally affects the nasal cavity and rarely the skin. Sporadic involvement of gastrointestinal tract and testis has been reported.[1] Patients are usually adult males presenting with a short history of fever, weight loss and fatigue. Multiple tumor-like lesions affect the trunk or extremities. In a study evaluating the clinical and histologic features of cutaneous extranodal natural killer T-cell lymphoma nasal type, purpuric, abscess-like and nodular presentations have been reported in equal proportions (in about one-third cases each).[2] Extranodal natural killer T-cell lymphoma nasal type lesions show a dermal infiltrate of small-, medium- or large-sized pleomorphic cells. Epidermal and subcutaneous involvement may also be present. Associated angioinvasion, necrosis and infiltrate of inflammatory cells may be seen. Abscess-like lesions show larger sized tumor cells as compared to the other clinical subtypes.[2],[3] Immunohistochemically, the cells show positivity for cytoplasmic CD3, CD56 and granzyme B.[1],[4]
Many cutaneous lymphomas can show a T-cell phenotype and mimic extranodal natural killer T-cell lymphoma nasal type on histology. These are differentiated on the basis of clinical findings and immunohistochemistry studies.[1],[4] Mycosis fungoides usually shows an indolent course with progression over several years, unlike extranodal natural killer T-cell lymphoma nasal type. The presence of patch and plaque stages before the tumor stage is the norm in mycosis fungoides and the diagnosis of mycosis fungoides should be doubted in their absence. These lesions generally occur on the buttocks and covered areas of the body. Mycosis fungoides can be differentiated from extranodal natural killer T-cell lymphoma nasal type with the help of several features [Table - 1]. Subcutaneous panniculitis-like T-cell lymphoma usually present in adults with systemic symptoms of fever and weight loss similar to extranodal natural killer T-cell lymphoma nasal type. However, nodular, solitary or multiple lesions are seen to affect the legs in the former. The infiltrate is generally limited to the subcutaneous tissue and spares the epidermis and dermis, unlike extranodal natural killer T-cell lymphoma nasal type. The cells in subcutaneous panniculitis-like T-cell lymphoma express CD3 and CD8 but not CD56 as opposed to extranodal natural killer T-cell lymphoma nasal type.[1] Primary cutaneous acral CD8+ T-cell lymphoma is a new entity recently introduced in the World Health Organization classification. The lesions are localized to the face and extremities and are slowly progressive. The cellular infiltrate is CD3 and CD8 positive but has a low Ki-67 proliferation index with absence of epidermotropism thus distinguishing it from extranodal natural killer T-cell lymphoma nasal type.[4],[5] Cutaneous gamma-delta T-cell lymphoma is another aggressive lymphoma which can present with tumor-like lesions on extremities which is Epstein–Barr virus negative. Although gamma-delta T-cell receptor analysis could not be done in our case, the presence of large blastic cells on HPE and positive Epstein–Barr virus serology clinched our diagnosis as extranodal natural killer T-cell lymphoma nasal type. (Gamma-delta T-cell lymphoma has smaller cells).[1]

The prognosis of cutaneous lymphomas is widely variable and hence mandates correct tumor typing. As the clinical course in extranodal natural killer T-cell lymphoma nasal type is fulminant, systemic chemotherapy is generally instituted even in lesions localized to the skin. However, failure rates are high and overall survival is poor. Median survival of less than a year is seen in patients with metastatic disease involving extracutaneous organs. In mycosis fungoides, the prognosis is stage dependent. Although the patch and plaque stages show near-normal life expectancy, presence of tumors and extracutaneous involvement worsens the prognosis. The prognosis of subcutaneous panniculitis-like T-cell lymphoma varies with its phenotype.[1]
In conclusion, it is important to remember that extranodal natural killer T-cell lymphoma nasal type may present acutely with systemic symptoms mimicking an abscess. Clinical correlation, histology and immunohistochemical studies are necessary to establish the correct diagnosis and initiate appropriate treatment to prevent the worsening of these aggressive lymphomas.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Willemze R, Jaffe ES, Burg G, Cerroni L, Berti E, Swerdlow SH, et al. WHO-EORTC classification for cutaneous lymphomas. Blood 2005;105:3768-85.
[Google Scholar]
|
| 2. |
Lee WJ, Lee MH, Won CH, Chang SE, Choi JH, Moon KC, et al. Comparative histopathologic analysis of cutaneous extranodal natural killer/T-cell lymphomas according to their clinical morphology. J Cutan Pathol 2016;43:324-33.
[Google Scholar]
|
| 3. |
Lee WJ, Jung JM, Won CH, Chang SE, Choi JH, Chan Moon K, et al. Cutaneous extranodal natural killer/T-cell lymphoma: A comparative clinicohistopathologic and survival outcome analysis of 45 cases according to the primary tumor site. J Am Acad Dermatol 2014;70:1002-9.
[Google Scholar]
|
| 4. |
Swerdlow SH, Jaffe ES, Brousset P, Chan JK, de Leval L, Gaulard P, et al. Cytotoxic T-cell and NK-cell lymphomas: Current questions and controversies. Am J Surg Pathol 2014;38:e60-71.
[Google Scholar]
|
| 5. |
Swerdlow SH, Campo E, Pileri SA, Harris NL, Stein H, Siebert R, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood 2016;127:2375-90.
[Google Scholar]
|
Fulltext Views
2,324
PDF downloads
1,946





![[Figure - 1]](#fig_ijdvl_2018_84_4_518_222314_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2018_84_4_518_222314_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2018_84_4_518_222314_f3.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2018_84_4_518_222314_t4.jpg){kind=link}