
Translate this page into:
Nail cosmetics: What a dermatologist should know!

Corresponding author: Prof. Archana Singal, Department of Dermatology and STD, University College of Medical Sciences and GTB Hospital, Dilshad Garden, Delhi, India. archanasingal@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Tyagi M, Singal A. Nail cosmetics: What a dermatologist should know! Indian J Dermatol Venereol Leprol. 2024;90:178–85. doi: 10.25259/IJDVL_77_2023
Abstract
Nail cosmetics industry is growing at an enormous rate globally due to a surge in nail care all around the world. Various nail cosmetics are available, such as nail polish along with its variants like shellacs, finishes, artificial nails, adornments, and nail polish removers. Nail cosmetics serve aesthetic as well as therapeutic purposes, with the end result being smooth, attractive nails. Nail grooming procedures have evolved from a basic manicure to many other advanced procedures like gel nails, nail tattooing, etc. Although a majority of nail cosmetics are considered safe, they may have potential complications, including allergic and irritant reactions, infections, and mechanical effects. The majority of the procedures related to nail enhancement are not performed by dermatologists but by beauticians with inadequate or no knowledge of the nail’s anatomy and functions. The hygiene at the so-called nail-salons/beauty parlours is not standardised, leading to acute complications like paronychia and nail dystrophy following matrix injury. The use of nail cosmetics has become widespread, making it essential for dermatologists to be aware of the nail care products, aesthetic procedures pertaining to nails, and related adverse effects.
Keywords
Nail cosmetics
nail polish
artificial nails
manicure
sculptured nails

Introduction
The nail is an opalescent window and functions as a vehicle for cosmetics and aesthetic manipulation. Nail cosmetics are used by millions of people worldwide, regardless of gender, who wish to have attractive, smooth, shiny, and adorned nails and the variety of products is expanding. Nail cosmetics are also used to hide diseased nails affected by various infectious and inflammatory nail pathologies that adversely affect self-esteem. Nail cosmetics are in a phase of constant evolution, with newer nail cosmetics, procedures, adornments flooding the market every other day. These procedures are often performed by the beauticians without sound knowledge of the anatomy and disease potential of the procedures, resulting in complications. Therefore, it is essential for the dermatologists to be familiar with the nail cosmetic products and procedures for better case management. In this review, we aimed to provide an update on nail cosmetics, nail procedures, and their potential complications.
Ideal nail
An ideal nail or nail which is considered attractive, generally depends on the trend. However, it often has an oval contour, glossy and translucent surface, tip extending beyond the nail with no overhanging cuticles, and no corners giving an illusion of long slender fingers or toes.
Impact of nail cosmetics on the global economy
There is a surge in the interest in nail care among the global population, mainly because of the product innovation, increased influence of social media, rising popularity among mature and older ages, and an increased number of working women along with more college going girls. The global nail care market is estimated to grow substantially in the coming 10 years from 10.9 billion USD in 2021 to 23.1 billion USD by the end of 2031 (The global nail care market, 2022).1 Among the nail care products, the nail polish segment accounts for the largest share owing to the variety and cost of the products. Similar trends are expected to dominate the Indian nail care market in the coming years.
History
The origin of nail coloring agents date back to 3000 B.C. and they were used as a distinction of rank and dynasty. Various ingredients were used for nail color like beeswax, Arabic gum, egg whites, heena, lavender oil, etc.2 Modern day nail polish was formulated in the 1920s and became commercially available in 1932 by the company now known as Revlon.3 In ancient times, artificial nails were worn by noblewomen as a sign of status and were made of bone, ivory and gold.4 In 1954, a dentist, Fred Slack, created an artificial nail using his dental equipment and chemicals. He experimented with different materials and patented a successful version using acrylics and started the company “Patti nails.” Over the time, the process has changed significantly.4
Types of nail cosmetics
Various types of nail cosmetics have been listed in Box 1. They not only improve the aesthetic appeal but also have the additional advantage of being used in diseased nails, for example transparent nail lacquer is used for brittle nails. They may be used as an adjuvant to medical treatment of mild nail dystrophy by hiding the lesions and buying time until nail manifestations resolve with the treatment. Though nail cosmetics are considered safe in general, they may be accompanied by complications.
Nail polish and its variants Nail shellacs Nail hardeners Nail polish finishes Nail polish removers Artificial nails: Nail tips Nail wraps and modifications Sculptured nails: Acrylic nails, gel nails Nail adornments Nail moisturisers
Various nail cosmetics shall be discussed one by one.
Nail polish: Nail polish (syn. nail paint, nail varnish) is a lacquer that is applied over nails for the purposes of beautification, strengthening and camouflaging.
Basics of nail cosmetic materials:5 The principles of nail cosmetic materials are based on adhesion, polymerization and evaporation.
-
Adhesion
Adhesion is an important step in nail enhancement, as it is what makes two surfaces stick together. Primers or base coats make the surface of the nail plate more compatible and resist the peeling of the product applied. It improves adhesion and requires a dry and clean surface to act well.
-
Polymerisation
It involves the application of a monomer and the use of initiators or energy sources for cross-linking molecules.
-
Evaporation
Polymers are dissolved in solvents that evaporate (like toluene), and the material hardens.
Variants of nail polish: 6 In addition to the conventional one, there are varieties of fashionable nail polish that are now commercially available[Table 2].
| Film-forming agents |
Nitrocellulose (major) Others: methacrylate polymers, vinyl polymers |
| Film-forming resins |
Used for adherence and prevent chipping. Commonly used agents: formaldehyde, polyamide, toluene-sulfonamide-formaldehyde (tosylamide-formaldehyde resin). TSFR can cause allergic contact dermatitis. |
| Plasticizers |
Keep product pliable and prevent chipping. Contain: diethylpthhalate, dibutylphthalate, dioctylphthalate, tricresyl phosphate and camphor. |
| Solvents |
Dry quickly to leave a colored film behind on the nail surface. Consist of acetates, toluene, xylene and alcohol. |
| Colorants |
Various organic and inorganic pigments are used and are primarily used in “lake” forms that is organic forms are absorbed into inorganic insoluble forms. Mineral pigments: zinc oxide, titanium oxide, iron oxides. Synthetic pigments: D and C red 6/7/19, FDC yellow. |
| Thickening agents | Clay derivatives used for uniform suspension of ingredients |
| Colour stabilizers7 |
Prevent ultraviolet (UV)-induced color fading. Contain-benzophenone-1 and etocrylene. |
| Other agents |
Guanine from fish scales, metal particles, titanium dioxide coated mica flakes, bismuth oxychloride; these ingredients can give different appearances. Metallic particles: aluminum, gold and silver give metallic shine. Light reflective ingredients: give pearl-like appearance or shimmer effects. Antifungal agents (ciclopirox 8%, amorolfine 5%): for therapeutic purposes. |
TSFR: Toluene-sulfonamide-formaldehyde resin
| Photochromatic | Ultraviolet sensitive compound which darkens on exposure to sunlight. |
| Thermochromatic |
Color change induced by temperature. Lighter color when cold and darker when fingers are warm. |
| Magnetic |
Contain iron powder. A magnet in the cap can be held close to the nail to formulate the iron powder in desired pattern before the evaporation of solvent. These should be removed before magnetic resonance imaging. |
| Breathable | Water and oxygen permeable. |
| Caviar | Small spherical beads pushed into wet nail polish to give a special effect. |
| Hypoallergenic8 | TSFR is the most common culprit for causing allergic contact dermatitis. Polyester resin or cellulose acetate butyrate may be used but sensitivity is still possible. Toxin-free nail polish does not contain dibutylphthalate, toluene and formaldehyde as publicised by some manufacturers. Hypoallergenic nail polish has increase polish peeling and therefore, are less popular. |
TSFR: Toluene-sulfonamide-formaldehyde resin
Nail shellac: 7,9 Nail shellac is a polish and gel hybrid that uses polymerization photo-initiators (different from gel nails) and acrylate oligo or monomers along with pigment from traditional nail lacquers. These require 6 coating steps, each of which is followed by exposure to light emitting diodes. These resist chipping and can be worn on natural nail plates. Nail shellacs are thinner and less heavy than gel nails and can be easily removed with acetone.
Nail hardeners: Nail hardeners are applied to strengthen soft and brittle nails. These contain formaldehyde which acts by cross linking keratin, but have the potential to cause paronychia, irritant dermatitis, onycholysis and chromonychia.10 Others may contain nylon, titanium-silicon-zirconium polymers, calcium, and biotin.11
Nail polish finishes: 5 Each finish contains special ingredients that determine the surface appearance and give a visual characteristic, for example, crème, shimmer, micro shimmer, matte, lustre, translucent, glitter, frost, duo-chrome, jelly, iridescent and opalescent.
Nail polish removers: Nail polish can be removed by redissolving the resin deposited on the nail plate after the solvent evaporates. Removers are applied with a tissue, cotton ball or they can be left on the nail and covered with aluminium foil. Acetone is most used, but its frequent use can cause dry lustreless nails and irritant dermatitis.
Acetone free removers contain ethyl acetate and butyl acetate.
Nail polish removal pads contain gamma butyrolactone, which can rarely get converted to gamma-hydroxybutyrate resulting in systemic toxicity.3 These can dehydrate and damage the nail.
Nail polish removers with fatty materials, lanolin, castor oil, cetyl palmitate and other synthetic oils, act as occlusive nail moisturisers. However, in practical use they are unable to overcome the dehydrating effect of the solvent.5
Artificial nails: Also known as false nails or nail enhancements, these are extensions placed to mimic the true nails or to have an artistic look. Artificial nails have versatility in size, design, shape and are placed over pre-existing nails.
Nail tips: Preformed tips, which can be pressed-on and pre-glued or unglued. The preformed tips are removed from the packaging, and placed on the nail plate, and held for a few seconds. These can be shaped and trimmed as desired. These are easily removed and last for a short term, usually less than a week.5 Traumatic removal can lead to onychoschizia. These are not very flexible and can cause onycholysis. Cyanoacrylate glues can cause allergic contact dermatitis.
Nail wraps and modifications: Linen, fiberglass or silk are applied to the natural nail plate using glue and over these acrylics are applied. Wraps provide strength. “No-light gels” consist of acrylate monomers thickened with polymers without reinforcing fabric.12
Sculptured nails: These are custom-designed nail elongations that fit according to individual requirements. These require a mixture of powder and a solution that is applied over the natural nail.
Acrylic nails: 9,12 A monomer like ethyl methacrylate is mixed with powdered polymethyl methacrylate polymer using benzoyl peroxide as an accelerator (coated over polymer powder) for polymerisation. Hydroquinone or monoethyl ether of hydroquinone can be added to slow down the process of polymerization. A template of foam is placed on a natural nail, and a new nail elongation is built over it. The powder mixture also contains additives like colorants. The acrylic slurry hardens in 2–3 minutes, after which it can be shaped, buffed, or covered with nail polish. The process of polymerization is fully complete in 24–48 hours. Acrylic nails can be removed with acetone and last for 3 weeks or longer with touch ups.
How to apply: A brush is dipped in liquid monomer and then passed through the polymer powder to form a small bead, which is applied over the natural nail plate. Three to six beads are brushed per nail plate. Photo-bonded nails are not popular due to adverse events such as photo-onycholysis and paresthesias. In these, acrylic nails are cured by a magnesium light for a few minutes.9
Gel nails: 3,9,12 Gel nails require ultraviolet (UV) light for hardening after application, which takes about 1–3 minutes. UVA lamps or light emitting diodes (LEDs) can be used for photocuring. Gel nails are composed of urethane acrylate oligomers, cross-linking monomers, photoinitiators and catalysts. These are applied in sequential coats (usually 3) and after each coat, photocuring is done. In the final steps, the nails are cleansed and shaping is done. Gel nails give high-gloss finish, more aesthetic appearance, have more strength, and does not chip [Figure 1]. Removal requires buffing, which, on repetition, can cause nail plate thinning. Touch ups are required every 3 weeks as with nail growth, a gap appears at the proximal end.

- Gel nails with nail art
Nail adornments: Multiple stickers, color strips, jewels or metal artefacts can be applied immediately before the polish dries and in various patterns followed by a top coat [Figure 2]. Nail designs can also be made after the first layer by making a design with a template in a different color.

- Artificial nails with nail adornments
Nail moisturisers: 12 These help with dry, brittle nails and are usually creams or lotions. Nail moisturisers contain occlusives, such as petrolatum, lanolin and humectants, such as glycerine and propylene glycol. Urea and alpha-hydroxy acids can be added to increase the water binding capacity of the nail plate. These work better if applied under occlusion at bedtime for at least 3 months.
Nail grooming procedures3,13
Manicure/Pedicure: It involves cleaning, shaping, and application of nail lacquer or artificial nails over finger nails (manicure) or toe nails (pedicure).
Steps of Manicure/pedicure
Hands /feet are soaked in warm water with soap to remove any debris and soften them to avoid onychoschizia during clipping.
Rough skin and thick callouses are buffed.
Nails are trimmed and filed to get the desired shape. Nails are shaped with no modification of corners to prevent ingrown nails.
A cuticle softener containing sodium and potassium hydroxide, quaternary ammonium compounds with urea is applied for 5–10 minutes (not recommended due to contact dermatitis and nail softening).
Cuticle is then pushed back using a metallic stick and trimmed; this step may damage the cuticle and thus predispose to infections especially, acute bacterial or fungal paronychia.
The surface of the nails are buffed with an emery board for a smooth appearance.
Hands and feet are dried and emollient cream is applied and massaged to soften the skin.
Application of nail lacquer or artificial nails.
Base coat: A transparent coat with high resin content for strong adhesion.
Nail polish: Many colors and types are available as discussed previously and can be applied in various styles.
Top coat: A transparent coat with more nitrocellulose which prevents chipping.
Other types of manicure: Other types of manicure depend on the final product applied, but the initial basic steps remain the same. These can be a shellac, gel or acrylic manicure, paraffin manicure, dip powder, Vinylux (Vinylux top coat nail polish with no base coat, strengthening with natural light, long lasting effect) manicure.
Medical tattooing
Medical tattooing, or dermopigmentation, is a process that involves the introduction of ink into the superficial layers of papillary dermis, to achieve a three-dimensional (3D) appearance of the nail bed and nail plate. This has been used for reconstruction of nail bed after the patient had bilateral surgical nail avulsion of both great toes to correct onychocryptosis or anonychia resulting from trauma or potentially dystrophic nail disorders like lichen planus of nails, surgical removal of nail unit tumuor using flaps. The skin surface is covered with a series of small dots applied next to each other to adapt to seasonal change and allowing recreation of shadows and highlights to produce a 3D effect.14
Therapeutic role of nail cosmetics in dermatology
Diseases involving the nails impair function, affect self-esteem, and adversely impact quality of life. Cosmetics can be used while awaiting therapeutic response or as prosthesis. Nail cosmetics can be helpful in disorders such as nail pitting, onychoschizia, senile onychorrhexia, brachyonychia, onychomycosis, mild nail dystrophy, dyschromias, onychotillomania, nail biting, habit tic deformity, ingrown toe nails, and anonychia.13 However, onycholysis and paronychia can be worsened by nail cosmetics. If sensitivity is present due to a product, it can exacerbate psoriasis due to Koebnerization. A study observed the photoprotective efficacy of opaque nail polishes can provide a sun protection factor of around 500 and can be useful in cancer patients on chemotherapeutic drugs which can affect nails.15
Adverse effects
Nail cosmetics and their associated procedures can be damaging to the natural nail. These adverse effects can be classified into those related to the procedures and salon services [Table 3] and due to the products like nail polish and artificial nails [Table 4]. Infections Paronychia, onycholysis, brittle nails and onychoschizia. Caused by nail polish removers, cuticle removers, primers, and nail hardeners. Frequent use of acetone and other alcohols along with vigorous rubbing and sodium and potassium hydroxide in cuticle removers can cause an irritant reaction. Presents with scaling, itching and burning, involve periungual tissue, onycholysis, nail bed hyperkeratosis, paronychia, splinter haemorrhages and nail dystrophy (Beau’s lines, ridging, rough lustreless nails). Distant involvement of face, especially around eyelids. Unusual involvement of genitals and perianal region has been reported.26
Seborrheic dermatitis like pattern of ACD has also been reported.27
Paronychia, onycholysis, nail dystrophy, pseudo-psoriatic nails. Airborne-Dermatitis over face or distant locations can also be involved due to airborne transit of nail polymerised resins that becomes depolymerized by filing or are not polymerised.28
Contact cheilitis has occurred due to unpolymerized methacrylate.29
‘The artificial nail grip sign’ is the name given to a pattern of ACD involving the proximal palm.30
Peripheral neuropathy- methyl methacrylate Recent study has reported that gel-based manicures can result in overestimation of actual readings. Therefore, it should be removed.35
No effect of regular nail polish. TSFR: Toluene-sulfonamide-formaldehyde resin, ACD: Allergic contact dermatitis, UV: Ultraviolet
Micro and macro trauma
Instruments and tools
Onychoschizia [Figures 3 and 4], thinning, and brittle nails
Clipping nails when dry and during removal process
Hapalonychia
Weak foldable nails due to filing, drilling, buffing
Onycholysis [Figure 5]
Repeated manicure/pedicure and probing under nails
Cuticle cutting and probing under nails, improper sterilisation of equipments, improper cleaning of pedicure footbaths
Nail plate thinning18
Overhydration due to stick-on dressing
Transverse leukonychia19
Repeated microtrauma during manicure
Nail polish
Discoloration of nail
Keratin staining mainly due to red (D and C red number 7,34,6) and yellow (FDC yellow number 5 lake), happens when the polish is left for more than 7 days, resolve on its own after removal in 2 weeks.
White striae on nail plate
Pseudo-leukonychia due to interaction of nail polish with keratin leading to keratin degranulation [Figure 6], can be confused with superficial white onychomycosis.
Irritant reaction
Allergic contact dermatitis (ACD)-formaldehyde, TSFR, and acrylates. Others can be nitrocellulose,22 dibutylphthalate23 D and C yellow 11,24 benzoyl peroxide,25 acrylates, nickel and cobalt in nail adornments. [Figure 7)]
Artificial nails
Burns
Methacrylates, if spilled can cause third degree burns
Traumatic onycholysis
More common with acrylic nails (adhesion of acrylic nail to nail plate is stronger than adhesion of nail plate to nail bed).
Roller coaster nails
Oscillating pattern of the proximal border, along with pinpoint haemorrhages, occurs when patients insert a variety of thin and sharp objects into potential spaces.
Yellow, thin, and dry nails
Long-term use damaging the nail plate (not to be used consecutively for more than 3 months).
Nail matrix damage
Improper technique and when liquid acrylic enters the proximal nail fold.
ACD-Liquid monomer (acrylates)
Contact vitiligo31
May occur due to adhesives used in artificial nails or nail extensions [Figure 8]
Rarely, acrylates can interfere with fast axonal transport32
Worn down nails or overfilled nails33
Distal thinning with triangular and half moon morphology forms a mirror image to the lunula. The overfilled portion appears red and the plate is thinned.
UV-light related concerns
Ocular side effects are largely unknown. However, some dermatologists recommend UV filtered glasses if frequently using photo-manicures. Studies have established very low risk of malignancy, but some recommend using gloves to prevent photoaging. Three cases of squamous cell carcinoma have been reported with delay of 11 to 15 years in diagnosis after UV exposure.34 UV light can cause onycholysis in patients taking phtosensitizing medications.
Pulse oximetry related concerns

Onychoschizia following frequent use of nail polish remover
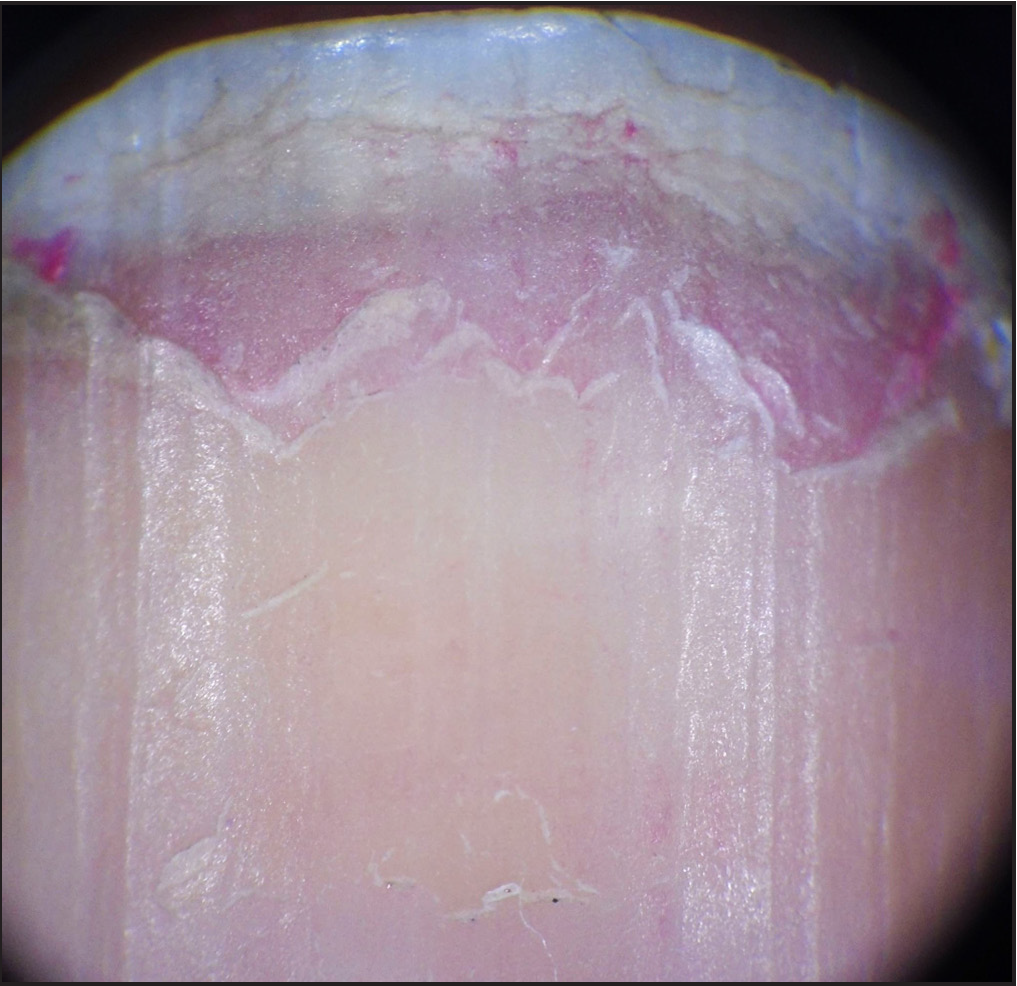
Onychoscopic image of onychoschizia; note pink colored remnants of nail polish. (Dermlite DL3 dermatoscope, polarised mode, 10x)

Onycholysis after manicure and probing under nails

Left toe with whitish keratin degranulation and right toe with greenish-yellow discoloration due to pseudomonas infection

Allergic contact dermatitis due to nail polish

Contact vitiligo on all fingers predominantly involving proximal nail folds and distal digits following use of artificial nail
Other reported side effects: Other rare side effects reported in the literature include bacterial endocarditis as a consequence of pedicure,36 candidal osteomyelitis and diskitis,37 pneumothorax and respiratory obstruction in a 15-month-old child due to accidental sucking of nail polish remover pads,38 pterygium inversum unguis,39 non-melanoma skin cancer.40
Testing for Allergic contact dermatitis (ACD) due to nail cosmetics3,4
Allergic contact dermatitis is the most encountered side effect of nail cosmetics and the following allergens should be tested
Formaldehyde: 1% in an aqueous solution.
Toluene-sulfonamide-formaldehyde resin (TSFR), dibutylphthalate, ethyl and butyl acetate: 5–10% of each in petrolatum.
Acetone3: 10% in olive oil, should be open patch test.
Acrylates should be tested with 2-hydroxy methacrylate, ethyl cyanoacrylate, and methyl methacrylate monomer-0.1–5% in petrolatum or olive oil.42
Importance/Concerns of nail cosmetics in healthcare settings
Long artificial nails and chipped nail polish can harbour pathogens like Candida, Klebsiella, Pseudomonas, which can be transmitted to patients if worn for a long time and are difficult to eliminate with antimicrobial soaps and sanitizers. A study showed that chipped nail polish or if it is worn for more than 4 days had increased bacteria on fingernails.43 Therefore, the nails should be kept short and unadorned.
Nail salon workplace hazards
Contact sensitization to chemicals and filings used in acrylic nail enhancement can occur. Nail technicians spend long hours in nail salons and in the process breathe dust particles and fumes, which can cause throat irritation as not all places are well ventilated. Occupational asthma can be a risk due to the use of cyanoacrylates.44
Patient information on safe use of nail salon and nail cosmetics3,13
The following information should be available to everyone who wishes to have a pleasant nail salon experience without complications.
Nail salon should be clean, and staff should be well attired with clean nails.
Ask about the sanitization and sterilisation of the salon.
Check the nail equipment; whether it has been cleaned and sterilised, and always try to carry personal equipment. Nail clippers, foot scrapers, callous removers and drills should be either autoclaved or soaked in hydrogen peroxide (7.5%) or glutaraldehyde (>2.4%) for 6 and 10 hours, respectively.
Wash hands before any services, and nails should be soaked for 10–20 minutes before cutting to prevent onychoschizia.
Cuticles should not be excessively pushed back, and nail plates should not be overbuffed.
Nail polish or artificial nails should be applied carefully so as not to enter proximal nail fold, which can cause damage to the nail matrix.
Extensions should be kept short.
Nail polish should only be left on for a few days and should not be layered over the old one. It should be removed with acetone-free cleansers.
If any nick or cut has occurred during the procedure, seek medical attention to prevent infections.
Wear gloves with wet work to protect the manicure.
If you experience any itching or burning after the service, it could indicate a reaction.
Seek medical attention, if any swelling, pain, redness and growths are present around the nails.
Conclusion
Nail cosmetics have become very popular and are being used widely. The products available are good for palliative treatment of nail disorders as well as for aesthetic purposes, but they are not devoid of adverse effects, especially allergic contact dermatitis. Therefore, knowledge of proper technique and the use of materials of standard quality is important. Dermatologists should be aware of the techniques, products and associated adverse events for their prompt identification and management and to facilitate appropriate advice on the safe and correct use of nail cosmetics/procedures.
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- The global nail care market is expected to grow rapidly for the next ten years. (2022, August 26). Retrieved from: https://www.premiumbeautynews.com/en/the-global-nail-care-market-is,20710.
- Nail polish. In Wikipedia. Retrieved October 5, 2022, from http://en.wikipedia.org/wiki/Nail_polish
- Nail cosmetics. Indian J Dermatol Venereol Leprol. 2012;78:309-17.
- [CrossRef] [PubMed] [Google Scholar]
- Artificial nails. In Wikipedia. Retrieved October 5, 2022, from https://en.wikipedia.org/wiki/Artificial_nails.
- Chapter 27: Colored nail cosmetics and hardeners. In: Draelos ZD, ed. Cosmetic Dermatology products and procedures (1st ed). Hoboken, NJ: Wiley-Blackwell; 2010. p. :206-13.
- [Google Scholar]
- Nail diseases related to nail cosmetics. Dermatol Clin. 2006;24:233-9.
- [CrossRef] [PubMed] [Google Scholar]
- Chapter 28: cosmetic prostheses as artificial nail enhancements. In: Draelos ZD, ed. Cosmetic Dermatology Products and Procedures (1st ed). Hoboken, NJ: Wiley-Blackwell; 2010. p. :215-21.
- [Google Scholar]
- Nail cosmetics in nail disorders. J Cosmet Dermatol. 2007;6:53-8.
- [CrossRef] [PubMed] [Google Scholar]
- Medical tattooing, the new frontiers: a case of nail bed treatment. Ann Ist Super Sanita. 2017;53:334-6.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of different nail polish in terms of photoprotective efficacy. Interest of their use as supportive care in patients with cancer. Bull Cancer. 2016;103:612-21.
- [CrossRef] [PubMed] [Google Scholar]
- An outbreak of furunculosis associated with foot-baths at a nail salon. N Engl J Med. 2002;346:1366-71.
- [CrossRef] [PubMed] [Google Scholar]
- Mycobacterium bolletii/Mycobacterium massiliense furunculosis associated with pedicure footbaths: a report of 3 cases. Arch Dermatol. 2011;147:454-8.
- [CrossRef] [PubMed] [Google Scholar]
- Side effects of nail cosmetics. J Cosmet Dermatol. 2005;4:204-9.
- [CrossRef] [PubMed] [Google Scholar]
- Transverse leuconychia induced by manicure: is there a contribution from dermoscopy? Pan Afr Med J. 2014;18:39.
- [CrossRef] [PubMed] [Google Scholar]
- Cosmetically Induced Disorders of the Nail with Update on Contemporary Nail Manicures. J Clin Aesthet Dermatol. 2016;9:39-44.
- [CrossRef] [PubMed] [Google Scholar]
- Nail cosmetics: a dermatological perspective. Clin Exp Dermatol. 2019;44:599-605.
- [CrossRef] [PubMed] [Google Scholar]
- Chapter 11: nail cosmetics. In: Rich P, Scher R, eds. An Atlas of Diseases of the Nail (1st ed). New York, NY: Parthenon Publishing; 2003. p. :97-100.
- [Google Scholar]
- A series of four cases of allergic contact dermatitis to phthalic anhydride/trimellitic anhydride/glycols copolymer in nail varnish. Contact Dermatitis. 2005;53:63-4.
- [CrossRef] [PubMed] [Google Scholar]
- Allergic contact cheilitis from D and C Yellow 11. Contact Dermatitis. 2009;60:294-5.
- [CrossRef] [PubMed] [Google Scholar]
- Contact dermatitis caused by benzoyl peroxide in podiatrists. Contact Dermatitis. 1999;40:163.
- [CrossRef] [PubMed] [Google Scholar]
- Frequency and main sites of allergic contact dermatitis caused by nail varnish. Dermatitis. 2008;19:319-22.
- [PubMed] [Google Scholar]
- ‘Seborrhoeic dermatitis’ of the head and neck without scalp involvement - remember nail varnish allergy. Contact Dermatitis. 2016;74:306-7.
- [CrossRef] [PubMed] [Google Scholar]
- Allergic contact dermatitis from sculptured acrylic nails: special presentation with an airborne pattern. Dermatol Reports. 2012;4:e6.
- [CrossRef] [PubMed] [Google Scholar]
- Recurrent cheilitis and lip oedema caused by (meth)acrylates present in ultraviolet-curable nail lacquer. Contact Dermatitis. 2015;72:341-2.
- [CrossRef] [PubMed] [Google Scholar]
- Palmar Eczema from Secondary 2-Hydroxyethyl Methacrylate Exposure-The Artificial Nail Grip Sign. Dermatitis. 2020;31:e26-e27.
- [CrossRef] [PubMed] [Google Scholar]
- A review of acrylates: Super glue, nail adhesives, and diabetic pump adhesives increasing sensitization risk in women and children. Int J Womens Dermatol. 2020;23;6:263-7.
- [PubMed] [Google Scholar]
- Fast axonal transport: a site of acrylamide neurotoxicity? Neurotoxicology. 2002;23:223-51.
- [CrossRef] [PubMed] [Google Scholar]
- Worn down nails after acrylic nail removal. Dermatol Online J. 2015;21 13030/qt15781m13037vc
- [PubMed] [Google Scholar]
- Side effects of gel nail polish: A systematic review. Clin Dermatol. 2022;40:706-15.
- [CrossRef] [PubMed] [Google Scholar]
- The effects of gel-based manicure on pulse oximetry. Singapore Med J. 2019;60:432-5.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- A forgotten but important risk factor for infective endocarditis in patients with prosthetic valve. Pedicure Scand J Infect Dis. 2007;39:274-6.
- [CrossRef] [PubMed] [Google Scholar]
- Candida osteomyelitis and diskitis after spinal surgery: An outbreak that implicates artificial nail use. Clin Infect Dis. 2001;32:352-7.
- [CrossRef] [PubMed] [Google Scholar]
- Acetone‐free nail polish removers: Are they safe? Clin Toxicol (Phila). 2005;43:297-9.
- [PubMed] [Google Scholar]
- Pterygium inversum unguis secondary to gel polish. J Eur Acad Dermatol Venereol. 2018;321:160-3.
- [CrossRef] [PubMed] [Google Scholar]
- Occurrence of nonmelanoma skin cancers on the hands after UV nail light exposure. Arch Dermatol. 2009;145:447-9.
- [CrossRef] [PubMed] [Google Scholar]
- Contact Sensitization to Allergens in Nail Cosmetics. Dermatitis. 2017;28:231-40.
- [CrossRef] [PubMed] [Google Scholar]
- The nail and cosmetics. In: Samman PD, Dav F, eds. The Nails in Disease (4th ed). Chicago: Year‐book Publishers; 1986. p. :129.
- [Google Scholar]
- Bacterial carriage on the fingernails of OR nurses. AORN J. 1994;60:796.
- [CrossRef] [PubMed] [Google Scholar]
- Occupational asthma caused by artificial cyanoacrylate fingernails. Ann Allergy Asthma Immunol. 2009;102:440-1.
- [CrossRef] [PubMed] [Google Scholar]




