Translate this page into:
Newer trends in the management of psoriasis at difficult to treat locations: Scalp, palmoplantar disease and nails
Correspondence Address:
Sanjeev Handa
Department of Dermatology, Venereology and Leprology, Postgraduate Institute of Medical Education and Research, Chandigarh - 160 012
India
| How to cite this article: Handa S. Newer trends in the management of psoriasis at difficult to treat locations: Scalp, palmoplantar disease and nails. Indian J Dermatol Venereol Leprol 2010;76:634-644 |
Abstract
Psoriasis is a common, chronic, inflammatory disease with a wide range of clinical presentations. The disease severity ranges from mild to severe. Plaque type of psoriasis is the most common. A number of factors like previous treatment history and comorbid conditions influence the treatment of psoriasis in an individual patient. Location of the lesions is also an important consideration. Psoriasis localized to certain areas of the body like scalp, nails, palms and soles remains difficult to treat. These sites have been referred to as the difficult locations in literature. This article covers the management of psoriasis limited to these special areas.Introduction
Psoriasis is a common, chronic, inflammatory, multisystem disease of the skin and joints, which accounts for 2.3% of the total dermatology outpatients in India. [1] A number of factors influence the treatment of psoriasis in an individual patient like site of lesions, treatment history, cost consideration and comorbid conditions. Psoriasis localized to certain areas of the body like scalp, nails, palms and soles calls for special intervention and remains difficult to control for various reasons like unrealistic expectations of the patients, time-consuming applications, side effects, cosmetic non-acceptability, restricted bioavailability of drugs and problems of adherence to treatment. [2] These sites have been referred to as the difficult locations in literature. [3] This article covers the management of psoriasis limited to these special areas. Topical treatment remains the first line of therapy for patients who present with an isolated involvement of these sites. However, in case of severe involvement of these sites or in patients who are refractory to topical therapy, systemic therapy is warranted.
Scalp Psoriasis
Scalp is the first site of involvement in up to 25% of the patients of psoriasis. [1] Up to 79% of patients of chronic plaque psoriasis may have scalp involvement. It can be mild to severe, and frequently itchy, cosmetically embarrassing and affects the quality of life adversely. The treatment of scalp psoriasis is beset with problems of drug delivery, facial irritation, messy, time-consuming, cosmetically unacceptable applications and staining of hair. Treatment is often prolonged. [1],[2],[3],[4],[5],[6],[7],[8],[9]
Medications for scalp psoriasis include those to be left on the scalp and the wash off products. Left on products are gels, lotions and ointments containing steroids, coal tar, salicylic acid or vitamin D analogs. Wash off products are shampoos containing coal tar, salicylic acid, sulfur, selenium, ketoconazole or zinc pyrithione. Van de Kerkhof et al. [8] divided the treatment of scalp psoriasis into four phases. First phase involves descaling using salicylic acid or urea preparations. The second phase is the clearing phase in which topical corticosteroids, vitamin D analogs, tar, dithranol, antifungal treatment, ultraviolet B light therapy or systemic treatment are used. The third phase is stabilization using a steroid-sparing vitamin D analog during the week and a super potent topical corticosteroid at weekends. Finally, the fourth phase is maintenance, using a vitamin D analog alone or with a tar shampoo.
Corticosteroids
Topical corticosteroids are the recommended first-line therapy for short-term use. Response to treatment is quick but the potential for side effects, such as atrophy, striae, telangiectasias and tachyphylaxis, limits the duration of use. These side effects, though mentioned, are virtually never seen in the scalp. Use of potent steroids (twice a day) should be limited to 4 weeks as safety of use beyond 4 weeks is not established. The choice of preparation such as ointment, cream, gel, lotion, foam, spray or shampoo is mostly patient driven. The lowest strength preparation that allows for clinical clearing in an individual patient should be used for the shortest time, considering the possible side effects and tachyphylaxis. However, long-term use of mid-potency preparations or intermittent use of potent steroids is more commonly practiced by physicians. Clobetasol propionate (CP) 0.05% and betamethasone dipropionate 0.05% are among the most potent topical corticosteroid preparations currently used. Intralesional corticosteroids are used exceptionally for one to two localized patches not responding to topical steroids. [10],[11],[12],[13],[14],[15],[16],[17],[18],[19],[20]
Foam vehicles are the new alternatives to traditional topical preparations due to the advantage of minimal residue and increased ease of application. They are absorbed more rapidly, have a higher bioavailability, are not associated with suppression of the hypothalamic pituitary adrenal (HPA) axis, and once-daily administration has been seen to be as effective as twice daily administration. They are also associated with better compliance. CP foam 0.05% is generally as effective as CP solution for scalp psoriasis and may produce superior results against scaling. Dose is limited to 50 g/week. Mid-potency corticosteroid betamethasone valerate (BMV) has also become available in a new thermolabile, low-residue foam vehicle, BMV 0.12% foam. BMV foam produced greater improvement in the primary signs of scalp psoriasis than BMV lotion, placebo or other standard topical therapies. [16],[17],[18],[19]
Shampoo preparations are another new development. When clobetasol shampoo 0.05% was tried in a patient experience program, 50% of the patients said that the shampoo was easy to use and did not interfere with their daily routine. Almost 90% of patients found the shampoo better than other prescriptions they had used before for their scalp psoriasis. [20]
Non-steroidal topical preparations
Calcipotriene/calcipotriol
These are vitamin D 3 derivatives used for chronic, moderately severe psoriasis of the scalp. The 0.005% solution is applied to the affected area and rubbed gently into the scalp twice daily. Response to therapy takes about 8 weeks. It is not recommended in patients with acute psoriatic eruptions of the scalp, those with hypercalcemia or hypervitaminosis D. The main side effects are burning, itching, irritation and dryness. Irritation tends to decrease with time. Clearance has been observed after 8 weeks of once-daily treatment in up to 60% of patients. [21],[22],[23]
Anthralin
Anthralin 0.1-3% cream has been used for long-term treatment of scalp psoriasis. Concentration of the cream should be gradually increased according to the body response and tolerance of the patient. Anthralin is applied in a thin layer to the psoriatic area once daily, rubbed in well and left on the scalp for 5-10 minutes before washing with a shampoo and rinsing well. It is not used for acutely inflamed scalp psoriasis. Redness or irritation of the treated scalp is common. Anthralin may temporarily stain the fingernails, gray/white hair, skin and fabrics. Caution is advised in patients having history of allergy to anthralin or to preservatives (e.g., parabens). [6]
Coal tar
Coal tar is an effective and a cheap treatment modality for scalp psoriasis. Staining and a pungent odor are the problems associated with its use. Topical tar solution [liquor picis carbonis (LPC) or liquor carbonis detergens (LCD)] is widely available and commonly used for scalp psoriasis. Newer preparations specifically meant for scalp include coconut oil compound ointment (coal tar solution with precipitated sulfur, salicylic acid, coconut oil, yellow soft paraffin and emulsifying wax) and tar pomades (contain LCD, Tween 20 and salicylic acid in a hydrophilic ointment). Compound ointment is applied once at night and washed off in the morning using the coal tar shampoo. [24],[25],[26],[27]
Coal tar shampoos contain 1-20% coal tar extract. They are used twice weekly. A tar blend 1% shampoo Polytar (Steifel, Johannesburg, South Africa) is made of coal tar, juniper tar (cade oil) and pine tar. In a comparative 4-week study of tar blend 1% shampoo (Polytar) and CP 0.05% shampoo (Clobex, Galderma, Ft. Worth, USA) in the treatment of scalp psoriasis, the corticosteroid shampoo was significantly more effective and also had more cosmetic acceptability. [27],[28]
Tazarotene
There are no controlled studies on the use of tazarotene in scalp psoriasis. The response to tazarotene (0.1%) is less as compared to topical calcipotriol or steroids but at the same time relapse rates are reported to be less as well. Dryness and irritation are the common side effects observed. [6],[29]
Combination therapies
Combining different therapies offer advantages over individual therapies by allowing for enhanced efficacy and minimizing toxicity. Corticosteroids, when combined with vitamin D analogs, minimize the irritation while the total amount of corticosteroids required is low. For the treatment of moderate to severe plaque psoriasis of the scalp, the fixed-combination suspension containing betamethasone 0.05% and calcipotriene 0.005% is used once daily. In a randomized, double-blind, controlled trial over 8 weeks, 71.2% patients achieved "absent" or "very mild" disease with the two-compound scalp formulation, compared to 64% with betamethasone dipropionate, 36.8% with calcipotriene and only 22.8% with the vehicle alone. Pruritus was the only adverse event reported. [30],[31],[32],[33],[34]
Topical steroids with PUVASOL gave better results; 37.3% clearance versus 13.3% with PUVASOL used alone in psoriasis of the scalp. [35] LPC 10% along with 2% salicylic acid in a cream base along with PUVASOL for 8 weeks gave a much better clearance rate than PUVASOL used alone. [36]
Tazarotene has also been found to be efficacious in combination with topical steroids and calcipotriol. [29]
Second line treatments for recalcitrant disease
These are used only when all topical treatments fail. No controlled studies exist regarding their use. These include phototherapy and systemic medications like methotrexate, retinoids, cyclosporine and biologics. They are used based on physician experience, choice and risk versus benefit ratio.
Phototherapy
Hair blocks adequate penetration of ultraviolet light. Better results are achieved with conventional UV units, if hair is parted in many rows or if the patient has thin hair or if the head is shaved. Hand-held devices (UV combs) deliver a higher intensity of UV light. There are reports of the use of targeted phototherapy with excimer laser which provides narrowband ultraviolet B (NB-UVB) (308 nm) phototherapy with a very high irradiance, allowing for a shorter treatment time. [37],[38],[39],[40]
Biologics
Efalizumab has been tried in a 12-week study in a dose of 1 mg/kg/week SC with a significant improvement. However, it has now been recommended for withdrawal in the European market due to adverse effects. [41]
Miscellaneous agents
Salicylic acid 5-10% is combined with other topical therapies as a keratolytic. Many topical treatments do not work well until the thick scales, which reduce the drug penetration, are removed. Urea 10% and lactic acid 10% have been used as scalp moisturizers. In resistant cases, topical imidazole derivatives are used at times to control the overgrowth of Pityrosporum in scalp psoriasis. [42]
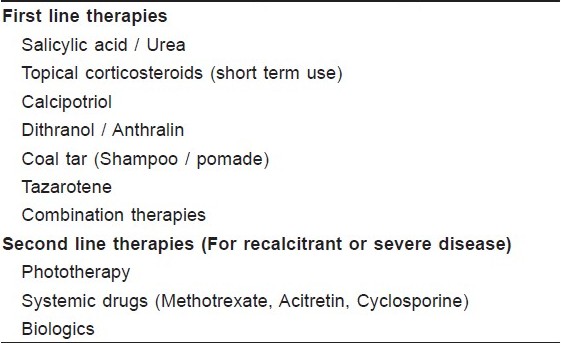
A simplified treatment algorithm is given in [Table - 1]. Despite the advances in drug delivery systems for scalp psoriasis, a lot still needs to be done. Better and well-tolerated treatment modalities for long-term use are urgently required.
Palmoplantar Psoriasis
Psoriasis exclusively involving the palms and soles is known as palmoplantar psoriasis. There are not many controlled clinical trials on the treatment of palmoplantar psoriasis in literature.
Palmoplantar psoriasis can present as hyperkeratotic plaques or as pustules. There is often overlap between the different morphological types. [43],[44] It is a difficult disease to manage. It leads to significant physical discomfort and dysfunction, resulting in disability. Reduction of pain and improvement in function may be more important therapeutic goals for patients than complete clearance. [45],[46]
Palmoplantar psoriasis is usually managed with topical therapy. Systemic therapy is used if the topical treatment fails or the disease is very severe. Though there are no validated scores with cut-off values to define which patients are eligible for topical versus systemic therapy, a combination of several factors like the physical/emotional impact of the disease, risk/benefit ratio of treatment and patient education/preference is used to determine medication selection.
Traditional topical treatments for palmoplantar psoriasis include tar, salicylic acid and corticosteroids. Combinations of these agents often work better than each individual agent. General measures like use of moisturizers, mild soaps and soap substitutes help in preventing painful fissures. There are also reports in literature on the improvement in palmoplantar pustulosis (PPP) with cessation of smoking and surgical interventions like tonsillectomy and shunt surgeries. [47],[48],[49]
A Cochrane Review in 2006 on interventions for chronic PPP concluded that the ideal treatment for PPP remains elusive. It supported the use of systemic retinoids and oral PUVA. However, a combination of PUVA and retinoids was better than the individual treatments. The use of topical steroids under hydrocolloid occlusion was beneficial. Low dose cyclosporine, tetracycline and Grenz Ray therapy may be useful in treating PPP. Colchicine, topical PUVA and hydroxyurea were found ineffective. [50],[51]
Salicylic acid
It is a keratolytic agent used as an adjunct to other topical agents. For palmoplantar disease, cream and ointment preparations in varying concentrations are used. Combinations with topical corticosteroids are frequently used. Salicylic acid should neither be used in combination with calcipotriene as it deactivates the molecule nor be combined with ultraviolet B (UVB) as it blocks UVB penetration. [51]
Coal tar
In many countries, crude coal tar is still the mainstay of therapy for palmoplantar psoriasis due to its low cost and easy availability. The 1-5% crude coal tar ointment with petrolatum, starch and zinc oxide is commonly used. Salicylic acid 5-10% is often added as a keratolytic. Coal tar has antibacterial, antifungal, antipruritic and anti-inflammatory effects. [26],[52],[53],[54]
Tar is not acceptable to patients due to its messy application, odor and ability to stain clothes. Attempts have been made to improve drug delivery through liposomal preparations. Longer duration of use and occlusion increase the efficacy. Combined with a corticosteroid cream under occlusion, it has been found useful for palmoplantar psoriasis. [53],[54]
Topical steroids
Conventionally, potent to super potent steroids have been used for palmoplantar psoriasis for periods up to 6-8 weeks and sometimes even longer. Newer formulations being used now include BMV 0.12% foam (Luxiq; Connetics Corp., Palo Alto, CA, USA) and CP 0.05% foam (OLUX, Connetics Corp.). These foam formulations offer cosmetic advantages over traditional forms, including minimal residue after application, quick drying, ease of application and lack of fragrance. These advantages may lead to improved compliance and hence efficacy. [18],[55],[56]
Calcipotriol
Calcipotriene has also been seen to be effective in palmoplantar psoriasis. A regimen alternating calcipotriene and potent topical corticosteroids may be better. In a study of 39 patients with palmoplantar psoriasis to evaluate the efficacy of occlusive calcipotriol 50 μg/mg ointment versus nonocclusive therapy for 6 weeks, twice-weekly occlusive calcipotriol ointment was as effective as the twice-daily application. [57]
Topical corticosteroids in combination regimens
Topical corticosteroids are frequently used in combination with other agents like topical vitamin D analogs or calcineurin inhibitors, or in the case of extensive disease, with phototherapy and systemic drugs. The combination of a corticosteroid and a vitamin D analog is more potent with fewer side effects than either agent alone. Sequential treatment (topical corticosteroid initially followed by the vitamin D analog for long-term use) is seen to achieve rapid improvement in the lesions while assuring long-term safety. A high-potency corticosteroid-vitamin D analog combination product may improve adherence, although it does not appear to be as effective as a super potent corticosteroid used alone. [58],[59],[60]
Anthralin
Anthralin may be used for patients not responding to other topical therapies. Dithranol 1% ointment is applied for 2 hours over the plaques and then removed by wiping with a cloth. At night, a steroid salicylic acid combination may be used under occlusion. [61]
Occlusive agents
Plain as well as steroid impregnated tapes have been used for the treatment of palmoplantar psoriasis. Newer occlusive materials like the hydrocolloid dressing composed of a hydrocolloid layer on a flexible gas- and water-impermeable backing that adheres to the skin have been tried. The hydrocolloid layer consists of a water-soluble polymer, water, a water-retaining agent and adhesive. Studies in which topical steroids have been used under occlusion have confirmed the efficacy of this treatment regimen. Problems with hydrocolloid dressing include irritation, folliculitis, excessive sweating and koebnerization, besides a poor cosmetic appeal and cost. The Food and Drug Administration (FDA) has recently approved a hydrogel patch which consists of a hydrogel layer on a thin, skin-colored, flexible, impermeable urethane backing. The hydrogel layer contains more water than the previously mentioned hydrocolloid layer, which allows for greater skin hydration. Colaco et al. demonstrated that occlusion with a hydrogel patch for 8 weeks is safe and efficacious with topical corticosteroids, tacrolimus and combination corticosteroid/calcipotriene. Adverse events related to hydrogel dressing application included irritation (3%), purpura (2.3%) and pruritus (1.5%). [62],[63],[64]
In recalcitrant palmoplantar psoriasis phototherapy, photodynamic therapy (PDT), methotrexate, acitretin and cyclosporine are the other alternatives. There are few studies on the use of biologics in recalcitrant PP psoriasis.
Phototherapy
Its main drawback is inconvenience of use, repeated hospital visits and an increased risk of skin cancer. Both soak psoralen plus ultraviolet A (PUVA) and oral PUVA with 8-methoxypsoralen (8-MOP) have been successfully used for the treatment of recalcitrant palmoplantar psoriasis. In a randomized, half side comparison, a significantly better effect was seen in lesions treated with oral PUVA compared with bath PUVA in the first 4 weeks, but the former also had more systemic side effects (nausea and/or dizziness). In an attempt to curtail the side effects of systemic PUVA, soak PUVA twice- or thrice-weekly with 30-minute hand and/or foot soaks in 8-MOP, 2.5 mg/l, followed by UVA irradiation has shown good results. The mean number of treatments required for maximal improvement was 28 (range 14-43). UVA dosage per treatment varied from 3.5 to 17.5 J/cm 2 , and the range of cumulative UVA required for maximal improvement was 45-388 J/cm 2 with a mean of 165 J/cm 2 . The mean serum level of 8-MOP, 60 minutes after completion of hand and foot soaks, was 2.5 ± 0.5 ng/ml compared with 95.75 ± 10.43 ng/ml after oral 8-MOP, 0.5 mg/kg. [65]
In a left right comparison of bath-water delivery of 0.0003% 5-MOP and 8-MOP aqueous solutions in palmar psoriasis, both the therapies cleared palmar lesions but 8-MOP required more UVA irradiation (46.3 ± 21.0 J/cm 2 vs. 30.2 ± 21.5 J/cm 2 ) and more exposures (21.0 ± 6.0 J/cm 2 vs. 17.0 ± 5.0 J/cm 2 ). [66]
In a comparative study on the efficacy and safety of local NB-UVB phototherapy versus local psoralen plus ultraviolet A (PUVA) paint in patients with palmoplantar psoriasis unresponsive to conventional therapies in 25 patients over 9 weeks, the difference in clinical response between the two treatment modalities was statistically significant with the local PUVA faring better than the local NB-UVB. [67]
Photodynamic therapy
Mild to marked improvement has been reported in palmoplantar pustular psoriasis with PDT, using 20% 5-aminolaevulinic acid and a 630 ± 50 nm light-emitting diode device at a power density of 30 mW/cm 2 and fluence of 15 J/cm 2 . [68]
Methotrexate
Disabling palmoplantar psoriasis hindering daily activities is an indication for the use of methotrexate. This implies that adequate trial has been made with topical therapy and phototherapy. Satisfactory response is generally seen in 3-6 weeks following administration. It is given at a dose of 0.2-0.4 mg/kg PO/IM/week as a single weekly dose. [69],[70],[71]
Cyclosporine
It is indicated in adult, non-immunocompromised patients with severe, disabling, recalcitrant palmoplantar psoriasis. Given in a dose of 2.5-5.0 mg/kg/day in two-divided doses/day, the dose should be decreased by 0.5-1.0 mg/kg when hypertension or abnormal renal function test results are seen. There is no consensus on the duration of use, though US FDA has approved it for 1-year continuous treatment. [69],[71]
Retinoids
Retinoids modulate epidermal proliferation and differentiation and have immunomodulatory and anti-inflammatory activity. Acitretin 10-50 mg/day is used as a single dose. Acitretin monotherapy is less effective than other traditional systemic agents and the effect is dose related. The response is also relatively slow, with a 3- to 6-month period required to achieve a maximal response. Many patients do not tolerate the higher dosages of acitretin to achieve optimal results. [72],[73],[74]
Combination therapies
The obvious goal in combination therapy is improved efficacy and decreased toxicity of each individual agent. In retinoid plus PUVA (RePUVA) therapy, acitretin is given in low doses (0.2-0.5 mg/kg) for 7 days and then PUVA treatment is started three times per week. Upon clearance, acitretin can be withdrawn, and maintenance phototherapy with PUVA or, preferably, NB-UVB, can be continued. [75]
Monochromatic excimer light
Monochromatic excimer light (MEL) therapy has been observed to be efficacious and well tolerated in patients with palmoplantar psoriasis. In a study involving 15 patients, a 52.5% improvement in the mean severity index score was seen after 25 MEL treatments (once a week), with 6.7% achieving clearance. Side effects included pruritus, erythema and blister formation. [40],[76],[77]
Radiotherapy
Radiotherapy (RT) is used in refractory palmoplantar psoriasis. The optimal irradiation dose is unknown. While evaluating the outcome of RT in six patients of psoriasis of palms and/or soles, Sumila et al. [78] recommended a SD of 0.5 Gy twice a week up to a TD of 4-5 Gy. They found the improvement highly significant.
Second line systemic agents
Clinical situations like drug intolerance, adverse effects to conventional therapies or treatment resistant disease may warrant a trial with second line drugs like sulfasalazine, fumaric acid esters, hydroxyurea, azathioprine, leflunomide, mycophenolate mofetil, tacrolimus and 6-thioguanine. There are no specific guidelines for their use in palmoplantar psoriasis.
Biologics
These should be reserved for patients who either fail or cannot use other conventional topical and systemic treatments. Currently, the biologic agents approved by the US FDA for the treatment of psoriasis include alefacept, efalizumab, etanercept, infliximab and adalimumab, while ustekinumab has been recommended for approval. Some of them have been tried in PPP. [79],[80],[81],[82],[83],[84],[85]
Alefacept
It is a dimeric fusion protein. Alefacept given in doses of 15 mg IM once a week for 3 months leads to significant clinical improvement in patients with extensive and recalcitrant palmoplantar psoriasis. [79],[80],[81]
Etanercept
It has been seen to be efficacious and well tolerated in PPP at 24 weeks in a randomized, placebo-controlled study involving 15 patients who received subcutaneous injections of either etanercept 50 mg or placebo twice a week for 3 months. [82]
Guidelines regarding the use of biologics in palmoplantar psoriasis are needed because of reports of paradoxical induction of palmoplantar pustular psoriasis and plaque psoriasis in a significant number of patients treated with biologics, mostly with infliximab followed by etanercept and adalimumab. [86]
Other reported therapies
These include the topical calcineurin inhibitor, tacrolimus for palmoplantar pustular psoriasis, and oral itraconazole at a dose of 100 mg/day for 1 month, followed by 100 mg on alternate days for another month, with some benefit. [87],[88]
Nail Psoriasis
Nails can be involved in 50-80% of patients of psoriasis. Isolated nail involvement is seen in 5-10% of patients. [89],[90] Nail psoriasis has a significant impact on the quality of life, affecting activities like doing finer tasks, interfering with jobs, cosmetic handicap, emotional and social problems. Some patients complain of pain and altered touch sensation. [91]
Despite the advances in therapy for psoriasis vulgaris, the options for nail psoriasis are rather limited. The duration of treatment is often very long, and in many cases, the disease is refractory to treatment. Lack of clear evidence validating the efficacy of various treatments makes it difficult to select the optimal treatment. [3] This had been complicated in the past by the lack of a standardized assessment protocol. The Nail Psoriasis Severity Index (NAPSI) designed recently has helped to standardize the outcome assessment. [92],[93],[94] The nail is divided into quadrants, rated with a 0 or 1, based on the signs from involvement of the nail matrix and the nail bed. NAPSI ranges from 0 to 8 for one nail and from 0 to 160 for all 20 nails.
Recent reports highlight the importance of selecting modalities according to specific psoriatic nail features. [89],[95] For example, nail matrix involvement manifesting as pitting, trachyonychia, dystrophy and leukonychia should be treated with different modalities as compared to nail bed involvement manifested by onycholysis, subungual hyperkeratosis, oil drop and splinter hemorrhage.
A therapeutic algorithm has been suggested by Jiaravuthisan et al. [89] depending upon the involvement of few or many nails.
Psoriatic lesions in a few nails
Topical therapy
(a) Nail matrix involvement
- Intralesional steroids
- Tazarotene
- Topical potent steroids
(b) Nail bed involvement
- Calcipotriol and steroids
- Tazarotene
- Cyclosporine
Psoriatic lesions in many nails
Systemic therapy
- Infliximab
- Retinoids
General measures for nail psoriasis include protection of nails from injury by wearing gloves and application of emollient creams on the psoriatic skin of the hands and nail folds.
Topical therapies include corticosteroids, vitamin D analogs, tazarotene, anthralin, 5-fluorouracil, cyclosporine, keratolytics/debridement agents (urea-propylene glycol) and combination therapies. Soft X-rays have been used for very severe disease. Topical therapy is always desirable to avoid side effects associated with systemic therapy and to increase patient compliance. Management of nail psoriasis is plagued by problems of drug delivery to the site. Nail permeability is quite low and limits topical therapy to mild disease. Several factors affect ungual drug delivery, such as molecular size, hydrophilic or hydrophobic nature, charge and the vehicle. Permeation of the drug into the nail can be enhanced by iontophoresis or by formulating drugs with vehicles which enable high drug partition out of the vehicle and into the nail plate. Disrupting the nail plate prior to using a drug is another alternative. Physical techniques like nail abrasion, microporation or application of chemical agents may be used. [96] Systemic therapy remains the mainstay in extensive or recalcitrant nail disease.
Corticosteroids
Topical
Potent to very potent topical steroids have been tried once or twice a day for up to 9 months. Patients clip the detached nail plate and apply steroids to the nail bed, hyponychium and paronychial area. Improvement has been reported in both the nail bed and the nail matrix features. Side effects include telangiectasias, atrophy of the paronychial area, and rarely, the corresponding phalanx. Recently, 8% clobetasol-17-propionate in a colorless nail lacquer vehicle used once daily for 21 days and then twice weekly for 9 months has shown good results. Nail parameters that responded best to therapy were onycholysis, pitting and salmon patches including nail pain. Response was directly related to the duration of therapy. [97],[98]
Intralesional steroids
Triamcinolone acetonide 0.05-0.1 ml of a 10 mg/ml solution is injected bimonthly at four injection sites: proximal nail fold area for nail matrix and the lateral nail folds for nail bed treatment for 5-6 months. Dermojet decreases pain but inclusion cysts have been reported even with dermojet. Side effects include Beau′s lines, proximal nail fold hypopigmentation, atrophy and subungual hematoma. Up to 70-90% of psoriatic patients with both nail matrix and nail bed lesions respond to intralesional steroids. Onycholysis is more difficult to treat, with only 20-55% of response. [99],[100],[101],[102],[103]
Tazarotene gel
Tazarotene 0.1% gel or cream applied once daily for 12-24 weeks has been shown to improve onycholysis, hyperkeratosis, pitting and salmon patches on both fingernails and toenails. A significant improvement in onycholysis was reported with tazarotene 0.1% gel. Improvement was faster in patients using it under occlusion. Tazarotene may cause mild skin irritation and burning or desquamation of the paronychial area. A lesser strength 0.05% has been used in children. [97],[104],[105],[106]
Vitamin D analogs
Calcipotriol twice daily application for 3-6 months has been evaluated in the treatment of nail psoriasis. In a study of 24 patients who used calcipotriol ointment (50 μg/g) on the affected nails twice daily without occlusion for 3 months, it was particularly effective in subungual hyperkeratosis, onycholysis and discoloration. [107],[108],[109],[110]
Topical cyclosporine solution
Cyclosporine is highly lipophilic in nature. Application of 70% maize-oil-dissolved oral cyclosporine solution when applied twice daily for 12 weeks has been reported to improve subungual hyperkeratosis and onycholysis in a randomized, placebo-controlled study. There were no reported adverse events. [111]
Combination therapy
Calcipotriol has been used in combination with steroids, with good results. Combined treatment with 8% clobetasol-17-propionate in lacquer applied at the weekend and tacalcitol ointment under occlusion on weekdays for 6 months has shown a good and quick response; response was related to length of therapy. The modified target NAPSI fell by 78% compared to baseline levels and the nail pain was also reduced. [109],[112]
Soft X-rays
Soft X-rays have been used for very thick nails in fractionated doses of 1.5 Gy for a total of 13.5 Gy (43 kV, 25 mA, 0.6 mm aluminum filter) at 1- and 2-week intervals. The nail plates normalized after 12 months of therapy. [113]
Systemic treatments that have been tried for nail psoriasis include retinoids, cyclosporine, fumaric acid esters, methotrexate, PUVA and biologics.
Acitretin
Results from an open study in patients with moderate to severe isolated nail psoriasis treated with low-dose acitretin at 0.2-0.3 mg/kg/day for 6 months show that the NAPSI score reduction was comparable to biologics at 41%. Complete resolution was seen in 25% of the patients, moderate improvement in 25% and mild improvement in 33% of the patients. [114],[115]
Cyclosporine
Cyclosporine has been used in a low dose (3.0 mg/kg/day) for nail psoriasis. A combination of systemic cyclosporine with topical calcipotriol twice a day for 3 months showed a better overall result in both mild and severe nail psoriasis. Improvement was noted in 79% of patients in the combination group versus 47% in patients using cyclosporine alone. [116],[117]
Fumaric acid esters have also been used in nail psoriasis with some success. [118] Methotrexate and PUVA are other systemic modalities used in recalcitrant cases.
Fungi may play a role in psoriatic nails. About one-third of the people who have nail psoriasis also have a fungal infection. Systemic antifungal treatment may at times be indicated. [119]
Biologics
Infliximab appears to be the most effective treatment for nail psoriasis to date. There are a few clinical trials specifically on nail psoriasis. Nails have been assessed in clinical trials for cutaneous psoriasis. A double-blind, placebo-controlled study of infliximab administered as a brief induction regimen at weeks 0, 2, and 6, followed by a single infusion every 8 weeks, revealed statistically significant mean percent improvement of 57.2% in the NAPSI score over placebo at week 24. Alefacept and efalizumab are the other biologics, which have been tried. [120],[121],[122]
| 1. |
Kaur I, Handa S, Kumar B. Natural history of psoriasis: a study from the Indian subcontinent. J Dermatol 1997;24:230-4.
[Google Scholar]
|
| 2. |
van de Kerkhof PC, Franssen ME. Psoriasis of the scalp. Diagnosis and management. Am J Clin Dermatol 2001;2:159-65.
[Google Scholar]
|
| 3. |
Wozel G. Psoriasis treatment in difficult locations: scalp, nails, and intertriginous areas. Clin Dermatol 2008;26:448-59.
[Google Scholar]
|
| 4. |
Farber EM, Nall L. Natural history and treatment of scalp psoriasis. Cutis 1992;49:396-400.
[Google Scholar]
|
| 5. |
van de Kerkhof PC, de Hoop D, de Korte J, Kuipers MV. Scalp psoriasis, clinical presentations and therapeutic management. Dermatology 1998;197:326-34.
[Google Scholar]
|
| 6. |
Chan CS, Van Voorhees AS, Lebwohl MG, Korman NJ, Young M, Bebo Jr BF, et al. Treatment of severe scalp psoriasis: From the Medical Board of the National Psoriasis Foundation. J Am Acad Dermatol 2009;60:962-71.
[Google Scholar]
|
| 7. |
Papp K, Berth-Jones J, Kragballe K, de la Brasinne M. Scalp psoriasis: A review of current topical treatment options. J Eur Acad Dermatol Venereol 2007;21:1151-60.
[Google Scholar]
|
| 8. |
van de Kerkhof PC, Kleinpenning M, Gerritsen R. Scalp psoriasis. In: Koo J, Lee CS, Lebwohl M, editors. Mild-To-Moderate Psoriasis. 2 nd ed. London: Informa Healthcare; 2009.
[Google Scholar]
|
| 9. |
Chen SC, Yeung J, Vhren MM. Scalpdex: A quality of-life instrument for scalp dermatitis. Arch Dermatol 2002;138:803-7.
[Google Scholar]
|
| 10. |
Reid DC, Kimball AB. Clobetasol propionate foam in the treatment of psoriasis. Expert Opin Pharmacother 2005;6:1735-40.
[Google Scholar]
|
| 11. |
Mazzotta A, Esposito M, Carboni I, Schipani C, Climenti S. Clobetasol propionate foam 0.05% as a novel topical formulation for plaque-type and scalp psoriasis. J Derm Treat 2007;18:84-7.
[Google Scholar]
|
| 12. |
Olsen EA, Cram DL, Ellis CN, Hickman JG, Jacobson C, Jenkins EE, et al. A double-blind, vehicle-controlled study of clobetasol propionate 0.05% (Temovate) scalp application in the treatment of moderate to severe scalp psoriasis. J Am Acad Dermatol 1991;24:443-7.
[Google Scholar]
|
| 13. |
Katz HI, Lindholm JS, Weiss JS, Shavin JS, Morman M, Bressinck R, et al. Efficacy and safety of twice daily augmented betamethasone dipropionate lotion versus clobetasol propionate solution in patients with moderate-to-severe scalp psoriasis. Clin Ther 1995;17:390-401.
[Google Scholar]
|
| 14. |
Jarratt M, Breneman D, Gottlieb AB, Poulin Y, Liu Y, Foley V. Clobetasol propionate shampoo 0.05%: A new option to treat patients with moderate to severe scalp psoriasis. J Drugs Dermatol 2004;3:367-73.
[Google Scholar]
|
| 15. |
Hogan DJ, Rooney ME. Facial telangiectasia associated with long-term application of a topical corticosteroid to the scalp. J Am Acad Dermatol 1989;20:1129-30.
[Google Scholar]
|
| 16. |
Feldman SR, Sangha N, Setaluri V. Topical corticosteroid in foam vehicle offers comparable coverage compared with traditional vehicles. J Am Acad Dermatol 2000;42:1017-20.
[Google Scholar]
|
| 17. |
Franz TJ, Parsell DA, Myers JA, Hannigan JF. Clobetasol propionate foam 0.05%: A novel vehicle with enhanced delivery. Int J Dermatol 2000;39:535-9.
[Google Scholar]
|
| 18. |
Stein L. Clinical studies of a new vehicle formulation for topical corticosteroids in the treatment of psoriasis. J Am Acad Dermatol 2005;53:S39-49.
[Google Scholar]
|
| 19. |
Feldman SR, Housman TS. Patients' vehicle preference for corticosteroid treatments of scalp psoriasis. Am J Clin Dermatol 2003;4:221-4.
[Google Scholar]
|
| 20. |
Johnson LA. P.O.W.E.R. (providing outcomes with effective results) in the shower-A patient experience program examining scalp psoriasis treatments. J Am Acad Dermatol 2007;56:AB188.
[Google Scholar]
|
| 21. |
Green C, Ganpule M, Harris D, Kavanagh G, Kennedy C, Mallett R, et al. Comparative effects of calcipotriol (MC 903) solution and placebo (vehicle of MC 903) in the treatment of psoriasis of the scalp. Br J Dermatol 1994;130:483-7.
[Google Scholar]
|
| 22. |
Thaci D, Daiber W, Boehncke WH, Kaufmann R. Calcipotriol solution for the treatment of scalp psoriasis: Evaluation of efficacy, safety and acceptance in 3,396 patients. Dermatology 2001;203:153-6.
[Google Scholar]
|
| 23. |
Barnes L, Altmeyer P, Forstrom L, Stenstrom MH. Long-term treatment of psoriasis with calipotriol scalp solution and cream. Eur J Dermatol 2000;10:199-204.
[Google Scholar]
|
| 24. |
Shah MK. Coconut oil compound ointment. Indian J Dermatol Venereol Leprol 2003;69:303-4.
[Google Scholar]
|
| 25. |
Kaur I, Saraswat A, Kumar B. A comparison of three therapeutic modalities in scalp psoriasis and a review of literature. Indian J Dermatol 2003;48:22-6.
[Google Scholar]
|
| 26. |
Paghdal KV, Schwartz RA. Topical tar: Back to the future. J Am Acad Dermatol 2009;61:294-302.
[Google Scholar]
|
| 27. |
Langner A, Wolska H, Hebborn P. Treatment of psoriasis of the scalp with coal tar gel and shampoo preparations. Cutis 1983;32:290-1, 295-6.
[Google Scholar]
|
| 28. |
Griffiths CE, Finlay AY, Fleming CJ, Barker JN, Mizzi F, Arsonnaud S. A randomized, investigator-masked clinical evaluation of the efficacy and safety of clobetasol propionate 0.05% shampoo and tar blend 1% shampoo in the treatment of moderate to severe scalp psoriasis. J Dermatolog Treat 2006;17:90-5.
[Google Scholar]
|
| 29. |
Lebwohl MG, Breneman DL, Goffe BS, Grossman JR, Ling MR, Milbauer J, et al. Tazarotene 0.1% gel plus corticosteroid cream in the treatment of plaque psoriasis. J Am Acad Dermatol 1998;39:590-6.
[Google Scholar]
|
| 30. |
van der Vleuten CJ, van de Kerkhof PC. Management of scalp psoriasis: guidelines for corticosteroid use in combination treatment. Drugs 2001;61:1593-8.
[Google Scholar]
|
| 31. |
Jemec GB, Ganslandt C, Ortonne JP, Poulin Y, Burden AD, de Unamuno P, et al. A new scalp formulation of Calcipotriene plus Betamethasone compared with its active ingredients and the vehicle in the treatment of scalp psoriasis: A randomized, double-blind, controlled trial. J Am Acad Dermatol 2008;59:455-63.
[Google Scholar]
|
| 32. |
Cassano N, Vena GA. Treatment of scalp psoriasis with betamethasone dipropionate and calcipotriol two-compound product. Acta Derm Venereol 2007;87:85-6.
[Google Scholar]
|
| 33. |
Downs AM. Dovobet ointment under occlusion overnight for troublesome scalp psoriasis. Acta Derm Venereol 2006;86:57-8.
[Google Scholar]
|
| 34. |
Buckley C, Hoffmann V, Shapiro J, Saari S, Cambazard F, Milsgaard M. Calcipotriol plus betamethasone dipropionate scalp formulation is effective and well tolerated in the treatment of scalp psoriasis: a phase II study. Dermatology 2008;217:107-13.
[Google Scholar]
|
| 35. |
Rama Sastry CV, Kar PK. A study of psoralen photochemotherapy with topical tar in the management of psoriasis vulgaris. Indian J Dermatol Venereol Leprol 2001;67:305-8.
[Google Scholar]
|
| 36. |
Kar PK, Rama Sastry CV. A study on combination therapy with PUVASOL and topical corticosteroid in psoriasis vulgaris involving scalp. Indian J Dermatol 2000;45:130-5.
[Google Scholar]
|
| 37. |
Taneja A, Racette A, Gourgouliatos Z, Taylor CR. Broad-band UVB fiber-optic comb for the treatment of scalp psoriasis: a pilot study. Int J Dermatol 2004;43:462-7.
[Google Scholar]
|
| 38. |
Morison WL, Atkinson DF, Werthman L. Effective treatment of scalp psoriasis using the excimer (308 nm) laser. Photodermatol Photoimmunol Photomed 2006;22:181-3.
[Google Scholar]
|
| 39. |
Mysore V. Targeted phototherapy. Indian J Dermatol Venereol Leprol 2009;75:119-25.
[Google Scholar]
|
| 40. |
Gattu S, Rashid RM, Wu JJ. 308-nm excimer laser in psoriasis vulgaris, scalp psoriasis, and palmoplantar psoriasis. J Eur Acad Dermatol Venereol 2009;23:36-41.
[Google Scholar]
|
| 41. |
Krell J, Nelson C, Spencer L, Miller S. An open-label study evaluating the efficacy and tolerability of alefacept for the treatment of scalp psoriasis. J Am Acad Dermatol 2008;58:609-16.
[Google Scholar]
|
| 42. |
Shemer A, Nathansohn N, Kaplan B, Weiss G, Newman N, Trau H. Treatment of scalp seborrheic dermatitis and psoriasis with an ointment of 40% urea and 1% bifonazole. Int J Dermatol 2000;39:532-34.
[Google Scholar]
|
| 43. |
Farber EM, Nall L. Nonpustular palmoplantar psoriasis. Cutis 1992;50:407-10.
[Google Scholar]
|
| 44. |
Kumar B, Saraswat A, Kaur I. Palmoplantar lesions in psoriasis: a study of 3065 patients. Acta Derm Venereol 2002;82:192-5.
[Google Scholar]
|
| 45. |
Farley E, Masrour S, McKey J, Menter A. Palmoplantar psoriasis: A phenotypical and clinical review with introduction of a new quality-of-life assessment tool. J Am Acad Dermatol 2009;60:1024-31.
[Google Scholar]
|
| 46. |
Pettey AA, Balkrishnan R, Rapp SR, Fleischer AB, Feldman SR. Patients with palmoplantar psoriasis have more physical disability and discomfort than patients with other forms of psoriasis: Implications for clinical practice. J Am Acad Dermatol 2003;49:271-5.
[Google Scholar]
|
| 47. |
Michaelsson G, Gustafsson K, Hagforsen E. The psoriasis variant palmoplantar pustulosis can be improved after cessation of smoking. J Am Acad Dermatol 2006;54:737-8.
[Google Scholar]
|
| 48. |
Ono T, Jono M, Kito M, Tomoda T, Kageshita T, Egawa K, et al. Evaluation of tonsillectomy as a treatment for pustulosis palmaris et plantaris. Acta Otolaryngol 1983;401:12-6.
[Google Scholar]
|
| 49. |
Hallberg D, Molin L. Remission of pustulosis palmaris et plantaris after intestinal shunt operation: reports on three cases. Acta Derm Venereol 1974;54:155-6.
[Google Scholar]
|
| 50. |
Marsland AM, Chalmers RJ, Hollis S, Leonardi-Bee J, Griffiths CE. Interventions for chronic palmoplantar pustulosis. Cochrane Database Syst Rev 2006;25:CD001433.
[Google Scholar]
|
| 51. |
Marsland AM, Griffiths CE. Treatments for chronic palmoplantar pustular psoriasis. Skin Therapy Lett 2001;6:3-5.
[Google Scholar]
|
| 52. |
Lin A, Moses K. Tar revisited. Int J Dermatol 1985;24:216-8.
[Google Scholar]
|
| 53. |
Goodfield M, Kownacki S, Berth-Jones J. Double-blind, randomized, multicenter, parallel group study comparing 1% coal tar preparation (Exorex) with a 5% coal tar preparation (Alphosyl) in chronic plaque psoriasis. J Dermatolog Treat 2004;15:14-22.
[Google Scholar]
|
| 54. |
Finlay AY, Young DW. Short contact crude coal tar therapy for psoriasis. Clin Exp Dermatol 1985;10:371-4.
[Google Scholar]
|
| 55. |
Givan J, Pearce D, Feldman SR. Topical corticosteroids. In: Koo JY, Lebwohl M, Lee CS, editors. Mild-to-Moderate Psoriasis. 2 nd ed. New York: Informa Healthcare; 2009. p. 23-39.
[Google Scholar]
|
| 56. |
Feldman SR, Horn EJ, Balkrishnan R, Basra MK, Finlay AY McCoy D, et al. Psoriasis: Improving adherence to topical therapy. J Am Acad Dermatol 2008;59:1009-16.
[Google Scholar]
|
| 57. |
Duweb GA, Abuzariba O, Rahim M, al-Taweel M, al-Alem S, Abdulla SA. Occlusive versus nonocclusive calcipotriol ointment treatment for palmoplantar psoriasis. Int J Tissue React 2001;23:59-62.
[Google Scholar]
|
| 58. |
Pearce DJ, Stealey KH, Balkrishnan R, Fleischer AB Jr, Feldman SR. Psoriasis treatment in the United States at the end of the 20th century. Int J Dermatol 2006;45:370-4.
[Google Scholar]
|
| 59. |
Lebwohl M, Siskin SB, Epinette W, Breneman D, Funicella T, Kalb R, et al. A multicenter trial of calcipotriene ointment and halobetasol ointment compared with either agent alone for the treatment of psoriasis. J Am Acad Dermatol 1996;35:268-9.
[Google Scholar]
|
| 60. |
Menter A, Abramovits W, Colσn LE, Johnson LA, Gottschalk RW. Comparing clobetasol propionate 0.05% spray to calcipotriene 0.005% betamethasone dipropionate 0.064% ointment for the treatment of moderate to severe plaque psoriasis. J Drugs Dermatol 2009;8:52-7.
[Google Scholar]
|
| 61. |
Van de Kerkhof PC. Dithranol treatment for psoriasis: after 75 years still going strong. Eur J Dermatol 1992;1:79-88.
[Google Scholar]
|
| 62. |
Shore RN. Clearing of psoriatic lesions after the application of tape. N Engl J Med 1985;312:246.
[Google Scholar]
|
| 63. |
Friedman SJ. Management of psoriasis vulgaris with a hydrocolloid occlusive dressing. Arch Dermatol 1987;123:1046-52.
[Google Scholar]
|
| 64. |
Colaco S, Fitzmaurice S, Becker E. New developments in topical psoriasis therapy: hydrogel patch. In: Koo JY, Lebwohl M, Lee CS, editors. Mild-to-Moderate Psoriasis. 2 nd ed. New York: Informa Healthcare; 2009. p. 165-82.
[Google Scholar]
|
| 65. |
Hofer A, Fink-Puches R, Kerl H, Quehenberger F, Wolf P. Paired comparison of bathwater versus oral delivery of 8-methoxypsoralen in psoralen plus ultraviolet: A therapy for chronic palmoplantar psoriasis. Photodermatol Photoimmunol Photomed 2006;22:1-5.
[Google Scholar]
|
| 66. |
Coleman WR, Lowe NJ, David M, Halder RM. Palmoplantar psoriasis: experience with 8-methoxypsoralen soaks plus ultraviolet A with the use of a high-output metal halide device. J Am Acad Dermatol 1989;20:1078-82.
[Google Scholar]
|
| 67. |
Sezer E, Erbil AH, Kurumlu Z, TaΊtan HB, Etikan I. Comparison of the efficacy of local narrowband ultraviolet B (NB-UVB) phototherapy versus psoralen plus ultraviolet A (PUVA) paint for palmoplantar psoriasis. J Dermatol 2007;34:435-40.
[Google Scholar]
|
| 68. |
Kim JY, Kang HY, Lee ES, Kim YC. Topical 5-aminolaevulinic acid photodynamic therapy for intractable palmoplantar psoriasis. J Dermatol 2007;34:37-40.
[Google Scholar]
|
| 69. |
Weinstein GD, Menter MA. An overview of psoriasis. In: Weinstein GD, Gottlieb AB, editors. Therapy of moderate-to-severe psoriasis. 2 nd ed. New York: Marcel Dekker; 2003. p. 1-29.
[Google Scholar]
|
| 70. |
Kalb RE, Strober B, Weinstein G, Lebwohl M. Methotrexate and psoriasis: 2009 National Psoriasis Foundation Consensus Conference. J Am Acad Dermatol 2009;60:824-37.
[Google Scholar]
|
| 71. |
Menter A, Korman NJ, Elmets CA, Feldman SR, Gelfand JM, Gordon KB, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis. Section 4. Guidelines of care for the management and treatment of psoriasis with traditional systemic agents. J Am Acad Dermatol 2009;61:451-85.
[Google Scholar]
|
| 72. |
Lassus A, Geiger JM. Acitretin and etretinate in the treatment of palmoplantar pustulosis: A double-blind comparative trial. Br J Dermatol 1988;119:755-9.
[Google Scholar]
|
| 73. |
Aydogan K, Karadogan SK, Tunali S. Acitretin-induced subungual hemorrhage. Int J Dermatol 2007;46:494-5.
[Google Scholar]
|
| 74. |
Schroder K, Zaun H, Holzmann H, Altmeyer P, el-Gammal S. Pustulosis palmo-plantaris: clinical and histological changes during etretin (acitretin) therapy. Acta Derm Venereol 1989;146:111-6.
[Google Scholar]
|
| 75. |
Ettler K, Richards B. Acitretin therapy for palmoplantar pustulosis combined with UVA and topical 8-MOP. Int J Dermatol 2001;40:541-2.
[Google Scholar]
|
| 76. |
Han L, Somani AK, Huang Q, Fang X, Jin Y, Xiang LH, et al. Evaluation of 308-nm monochromatic excimer light in the treatment of psoriasis vulgaris and palmoplantar psoriasis. Photodermatol Photoimmunol Photomed 2008;24:231-6.
[Google Scholar]
|
| 77. |
Nisticς SP, Saraceno R, Stefanescu S, Chimenti S. A 308-nm monochromatic excimer light in the treatment of palmoplantar psoriasis. J Eur Acad Dermatol Venereol 2006;20:523-6.
[Google Scholar]
|
| 78. |
Sumila M, Notter M, Itin P, Bodis S, Gruber G. Long-term results of radiotherapy in patients with chronic palmo-plantar eczema or psoriasis. Strahlenther Onkol 2008;184:218-23.
[Google Scholar]
|
| 79. |
Myers W, Christiansen L, Gottlieb AB. Treatment of palmoplantar psoriasis with intramuscular alefacept. J Am Acad Dermatol 2005;53:127-9.
[Google Scholar]
|
| 80. |
Guenther LC. Alefacept is safe and efficacious in the treatment of palmar plantar pustulosis. J Cutan Med Surg 2007;11:202-5.
[Google Scholar]
|
| 81. |
Jacobi A, Schuler G, Hertl M. Differential clinical response to alefacept in combination with methotrexate in two patients with refractory palmar psoriasis. Br J Dermatol 2007;156:178-80.
[Google Scholar]
|
| 82. |
Bissonnette R, Poulin Y, Bolduc C, Maari C, Provost N, Syrotuik J, et al. Etanercept in the treatment of palmoplantar pustulosis. J Drugs Dermatol 2008;7:940-6.
[Google Scholar]
|
| 83. |
Stinco G, Piccirillo F, Patrone P. Treatment of palmoplantar pustular psoriasis with efalizumab: A quick response with early recurrence. Eur J Dermatol 2008;18:91-2.
[Google Scholar]
|
| 84. |
Cohen DJ, Scherschun L. Case reports: Practical experience with efalizumab in hand and foot psoriasis. J Drugs Dermatol 2007;6:1224-30.
[Google Scholar]
|
| 85. |
Zip C. Treatment of hand and foot psoriasis with emphasis on efalizumab. Skin Therapy Lett 2007;12:7-9.
[Google Scholar]
|
| 86. |
Ko JM, Gottlieb AB, Kerbleski JF. Induction and exacerbation of psoriasis with TNF-blockade therapy: a review and analysis of 127 cases. J Dermatolog Treat 2009;20:100-8.
[Google Scholar]
|
| 87. |
Rivard J, Janiga J, Lim HW. Tacrolimus ointment 0.1% alone and in combination with medium-dose UVA1 in the treatment of palmar or plantar psoriasis. J Drugs Dermatol 2006;5:505-10.
[Google Scholar]
|
| 88. |
V'lckova-Laskoska MT, Caca-Biljanovska NG, Laskoski DS, Kamberova SJ. Palmoplantar pustulosis treated with itraconazole: A single, active-arm pilot study. Dermatol Ther 2009;22:85-9.
[Google Scholar]
|
| 89. |
Jiaravuthisan MM, Sasseville D, Vender RB, Murphy F, Muhn CY. Psoriasis of the nail: Anatomy, pathology, clinical presentation, and a review of the literature on therapy. J Am Acad Dermatol 2007;57:1-27.
[Google Scholar]
|
| 90. |
de Berker D. Management of psoriatic nail disease. Semin Cutan Med Surg 2009;28:39-43.
[Google Scholar]
|
| 91. |
de Jong EM, Seegers BA, Gulinck MK, Boezeman JB, van de Kerkhof PC. Psoriasis of the nails associated with disability in a large number of patients: Results of a recent interview with 1,728 patients. Dermatology 1996;193:300-3.
[Google Scholar]
|
| 92. |
Rich P, Scher RK. Nail Psoriasis Severity Index: a useful tool for evaluation of nail psoriasis. J Am Acad Dermatol 2003;49:206-12.
[Google Scholar]
|
| 93. |
Cassell SE, Bieber JD, Rich P, Tutuncu ZN, Lee SJ, Kalunian KC, et al. The modified Nail Psoriasis Severity Index: Validation of an instrument to assess psoriatic nail involvement in patients with psoriatic arthritis. J Rheumatol 2007;34:123-9.
[Google Scholar]
|
| 94. |
Kaηar N, Ergin S, Erdoan BS. The comparison of Nail Psoriasis Severity Index with a less time-consuming qualitative system. J Eur Acad Dermatol Venereol 2008;22:219-22.
[Google Scholar]
|
| 95. |
Cassell S, Kavanaugh AF. Therapies for psoriatic nail disease. A systematic review. J Rheumatol 2006;33:1452-6.
[Google Scholar]
|
| 96. |
Murdan S. Enhancing the nail permeability of topically applied drugs. Expert Opin Drug Deliv 2008;5:1267-82.
[Google Scholar]
|
| 97. |
Rigopoulos D, Gregoriou S, Katsambas A. Treatment of psoriatic nails with tazarotene cream 0.1% vs. clobetasol propionate 0.05% cream: A double-blind study. Acta Derm Venereol 2007;87:167-8.
[Google Scholar]
|
| 98. |
Sαnchez Regaρa M, Martνn Ezquerra G, Umbert Millet P, Llambν Mateos F. Treatment of nail psoriasis with 8% clobetasol nail lacquer: Positive experience in 10 patients. J Eur Acad Dermatol Venereol 2005;19:573-7.
[Google Scholar]
|
| 99. |
Grover C, Bansal S, Nanda S, Reddy BS. Efficacy of triamcinolone acetonide in various acquired nail dystrophies. J Dermatol 2005;32:963-8.
[Google Scholar]
|
| 100. |
de Berker DA, Lawrence CM. A simplified protocol of steroid injection for psoriatic nail dystrophy. Br J Dermatol 1998;138:90-5.
[Google Scholar]
|
| 101. |
Peachey RD, Pye RJ, Harman RR. The treatment of psoriatic nail dystrophy with intradermal steroid injections. Br J Dermatol 1976;95:75-8.
[Google Scholar]
|
| 102. |
Bleeker JJ. Intradermal triamcinolone acetonide treatment of psoriatic nail dystrophy with Port-o-Jet. Br J Dermatol 1975;92:479.
[Google Scholar]
|
| 103. |
Bedi TR. Intradermal triamcinolone treatment of psoriatic onychodystrophy. Dermatologica 1977;155:24-7.
[Google Scholar]
|
| 104. |
Scher RK, Stiller M, Zhu YI. Tazarotene 0.1% gel in the treatment of fingernail psoriasis: a double-blind, randomized, vehicle-controlled study. Cutis 2001;68:355-8.
[Google Scholar]
|
| 105. |
Bianchi L, Soda R, Diluvio L, Chimenti S. Tazarotene 0.1% gel for psoriasis of the fingernails and toenails: an open, prospective study. Br J Dermatol 2003;149:207-9.
[Google Scholar]
|
| 106. |
Diluvio L, Campione E, Paternς EJ, Mordenti C, El Hachem M, Chimenti S. Childhood nail psoriasis: A useful treatment with tazarotene 0.05%. Pediatr Dermatol 2007;24:332-3.
[Google Scholar]
|
| 107. |
Zakeri M, Valikhani M, Mortazavi H, Barzegari M. Topical calcipotriol therapy in nail psoriasis: A study of 24 cases. Dermatol Online J 2005;11:5.
[Google Scholar]
|
| 108. |
Tosti A, Piraccini BM, Cameli N, Kokely F, Plozzer C, Cannata GE, et al. Calcipotriol ointment in nail psoriasis: A controlled double-blind comparison with betamethasone dipropionate and salicylic acid. Br J Dermatol 1998;139:655-9.
[Google Scholar]
|
| 109. |
Rigopoulos D, Ioannides D, Prastitis N, Katsambas A. Nail psoriasis: A combined treatment using calcipotriol cream and clobetasol propionate cream. Acta Derm Venereol 2002;82:140.
[Google Scholar]
|
| 110. |
Tzung TY, Chen CY, Yang CY, Lo PY, Chen YH. Calcipotriol used as monotherapy or combination therapy with betamethasone dipropionate in the treatment of nail psoriasis. Acta Derm Venereol 2008;88:279-80.
[Google Scholar]
|
| 111. |
Cannavς SP, Guarneri F, Vaccaro M, Borgia F, Guarneri B. Treatment of psoriatic nails with topical cyclosporin: A prospective, randomized placebo-controlled study. Dermatology 2003;206:153-6.
[Google Scholar]
|
| 112. |
Sαnchez Regaρa M, Mαrquez Balbαs G, Umbert Millet P. Nail psoriasis: A combined treatment with 8% clobetasol nail lacquer and tacalcitol ointment. J Eur Acad Dermatol Venereol 2008;22:963-9.
[Google Scholar]
|
| 113. |
Rados J, Dobriζ I, Pasiζ A, Lipozenciζ J, Lediζ-Drvar D, Stajminger G. Normalization in the appearance of severly damaged psoriatic nails using soft x-rays. A case report. Acta Dermato venerol Croat 2007;15:27-32.
[Google Scholar]
|
| 114. |
Brazzelli V, Martinoli S, Prestinari F, Borroni G. An impressive therapeutic result of nail psoriasis to acitretin. J Eur Acad Dermatol Venereol 2004;18:229-30.
[Google Scholar]
|
| 115. |
Tosti A, Ricotti C, Romanelli P, Cameli N, Piraccini BM. Evaluation of the efficacy of acitretin therapy for nail psoriasis. Arch Dermatol 2009;145:269-71.
[Google Scholar]
|
| 116. |
Syuto T, Abe M, Ishibuchi H, Ishikawa O. Successful treatment of psoriatic nails with low-dose cyclosporine administration. Eur J Dermatol 2007;17:248-9.
[Google Scholar]
|
| 117. |
Feliciani C, Zampetti A, Forleo P, Cerritelli L, Amerio P, Proietto G, et al. Nail psoriasis: Combined therapy with systemic cyclosporin and topical calcipotriol. J Cutan Med Surg 2004;8:122-5.
[Google Scholar]
|
| 118. |
Vlachou C, Berth-Jones J. Nail psoriasis improvement in a patient treated with fumaric acid esters. J Dermatolog Treat 2007;18:175-7.
[Google Scholar]
|
| 119. |
Szepietowski JC, Salomon J. Do fungi play a role in psoriatic nails? Mycoses 2007;50:437-42.
[Google Scholar]
|
| 120. |
Noiles K, Vender R. Nail psoriasis and biologics. J Cutan Med Surg 2009;13:1-5.
[Google Scholar]
|
| 121. |
Kφrver JE, Langewouters AM, Van De Kerkhof PC, Pasch MC. Therapeutic effects of a 12-week course of alefacept on nail psoriasis. J Eur Acad Dermatol Venereol 2006;20:1252-5.
[Google Scholar]
|
| 122. |
Lamerson C, Stevens G, Sax K. Treatment of nail psoriasis with efalizumab: a preliminary study. Cutis 2008;82:217-20.
[Google Scholar]
|
Fulltext Views
14,027
PDF downloads
3,977





![[Table - 1]](#tbl_ijdvl_2010_76_6_634_72455_t1.jpg){kind=link}