Translate this page into:
NK/T-cell lymphoma nasal type with an unusual clinical course
2 4th Department of Medicine-Hematology, Faculty of Medicine, University Hospital in Hradec Kr�lov�, Charles University in, Czech Republic
3 Fingerland Department of Pathology, Faculty of Medicine, University Hospital in Hradec Kr�lov�, Charles University in, Czech Republic
Correspondence Address:
Vladimira Radochova
Sokolsk� 581, 50005 Hradec Kr�lov�
Czech Republic
| How to cite this article: Radochova V, Radocha J, Nova M, Belada D, Slezak R. NK/T-cell lymphoma nasal type with an unusual clinical course . Indian J Dermatol Venereol Leprol 2014;80:564-566 |
Sir,
Non-Hodgkin′s lymphomas present at an extranodal site in up to 40% of the patients. Extranodal nasal natural killer (NK)/T-cell lymphoma which represents about 1.4% of all lymphomas is more prevalent in East Asia and in certain parts of Central and South America and is frequently associated with Epstein-Barr virus (EBV) infection (60-90%). Most cases express CD56 (around 80%), CD2, granzyme B, and T-cell-restricted intracellular antigen-1 (more than 90%) and also carry p53 deletion. Systemic dissemination occurs later in the course of the disease. Patients with NK/T-cell lymphoma have a probability of survival at 5 years ranging from 37.9% to 43.5%. [1] We describe a patient with an unusual initial presentation and an unusual course during relapse.
A 56-year-old white man was referred for consultation regarding a lip swelling and non-healing wound after tooth extraction. One month prior to presentation, the patient underwent extraction of tooth 23 for the diagnosis of chronic periodontitis. However, soon afterwards, the patient developed a painless swelling of the lip, but he complained of mild pain during food intake in the area around the tooth extraction wound. He was treated with antihistaminic drugs without much relief. Almost simultaneously, erosions appeared on the mucosa around the extraction wound and on the palate. These lesions were sensitive after food intake. The patient denied any history of fever, weight loss, or nasal stuffiness. In addition, he had a history of arterial hypertension and had a 15-pack year history of smoking cigarettes. Examination revealed a swelling of the upper lip, which was soft and painless. The lymph nodes in the submandibular area were enlarged. Intraoral examination revealed a deep necrotic ulcer with a ragged border, measuring 20 mm in diameter, located on the left side of the hard palate. An erosion was present on the mucosa of the alveolar arch in the area of the wound [Figure - 1].
 |
| Figure 1: Ulcer after tooth extraction upon presentation |
Biopsy of the lesions showed ulcerated mucosa infiltrated with atypical lymphoid cells with angulated nuclei and bright cytoplasm with invasion into the surrounding tissues [Figure - 2]. Immunohistochemistry showed strong positivity for leukocyte common antigen, CD2, perforin, and granzyme B. Ki-67 showed a high proliferation activity of around 60%. EBV-encoded small RNA was negative. The diagnosis of NK/T-cell lymphoma nasal type was established. Since no other localization of lymphoma was seen during the initial staging (stage I E), the patient was treated with 6 cycles of CHOEP-14 (cyclophosphamide, doxorubicin, vincristine, etoposide, and prednisone) which led to partial remission. This was followed by field radiation therapy using intensity-modulated radiation therapy technique (27 × 2 Gy) which resulted in complete remission. Five months later, the patient was again admitted to the pulmonary department with fever and multiple pulmonary infiltrates [Figure - 3]. After the initial suspicion of pneumonia was ruled out, open lung biopsy was performed which confirmed early lung dissemination of the lymphoma. He was given salvage chemotherapy ESAP (etoposide, methylprednisolone, cytosine arabinoside, and cisplatin). However, despite therapy, the patient′s condition worsened, and he died 14 days later.
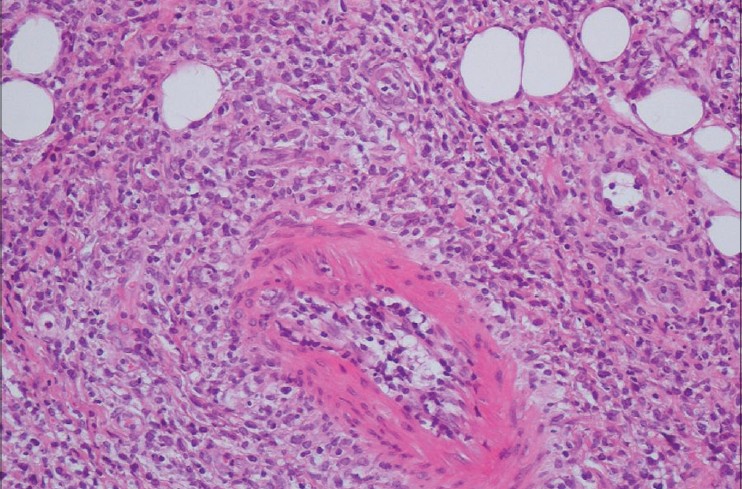 |
| Figure 2: Small lymphocytic infiltrates invading the tissue (H and E, ×200) |
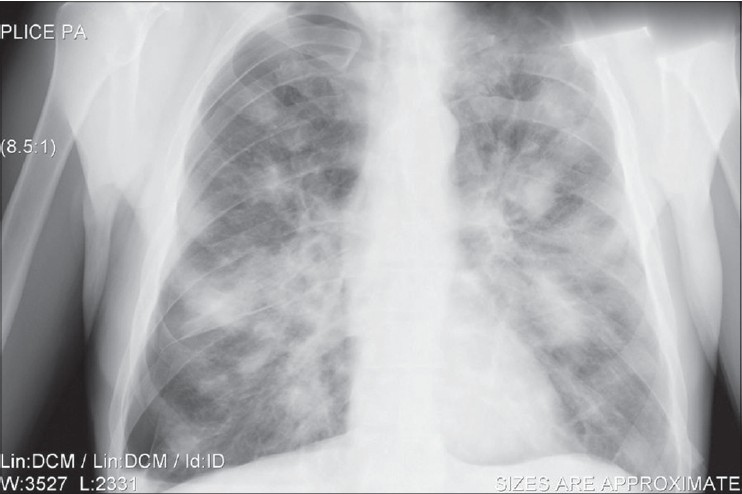 |
| Figure 3: Multiple nodular lymphoma infiltrates mimicking lung infection |
NK/T-cell lymphoma, nasal type has a very aggressive clinical course and a poor outcome. Involvement of the lung has been described only twice. [2],[3] We would like to stress this possible clinical feature of NK/T-cell lymphoma. Invasive diagnostic workup including biopsy of the lung is warranted in such cases in order to avoid misdiagnosis and delay in treatment. Palatal ulcers and non-healing ulcers in the oral cavity could represent a potentially malignant lesion which should warrant an immediate biopsy. It is frequently necessary to perform repeated examination before the diagnosis is made. In our patient, the palatal ulcer was first treated for suspected allergy and then as a wound after tooth extraction before he was referred to a specialized unit and biopsy was performed. In our case, CD56 was negative, but perforin and granzyme B were positive thus leading to the diagnosis. Current data suggest that many B-cell and some T-cell malignancies are associated with the presence of EBV in the tissue but this was not detected in our patient. According to a recent study, positron emission tomography/computerized tomography (PET/CT) is the preferred technique for imaging this type of lymphoma as it has significantly better sensitivity than conventional CT (97.7% vs. 80.7%, P < 0.001) and the findings can also affect the treatment plan and radiotherapy planning in more than 40% of patients. [4] Treatment consists of conventional CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone) or similar regimens followed by radiation therapy. Newer approaches may include asparaginase, gemcitabine or autologous stem cell transplantation. [5] The prognosis of this lymphoma remains poor. The 5-year disease free survival of nasal lymphoma is about 25% and the 2-year disease free survival in patients with extranasal lymphoma is about 10%.
| 1. |
Al-Hakeem DA, Fedele S, Carlos R, Porter S. Extranodal NK/T-cell lymphoma, nasal type. Oral Oncol 2007;43:4-14.
[Google Scholar]
|
| 2. |
Morovic A, Aurer I, Dotlic S, Weisenburger DD, Nola M. NK cell lymphoma, nasal type, with massive lung involvement: A case report. J Hematop 2010;3:19-22.
[Google Scholar]
|
| 3. |
Laohaburanakit P, Hardin KA. NK/T cell lymphoma of the lung: A case report and review of literature. Thora×2006;61:267-70.
[Google Scholar]
|
| 4. |
Moon SH, Cho SK, Kim WS, Kim SJ, Chan Ahn Y, Choe YS, et al. The role of 18F-FDG PET/CT for initial staging of nasal type natural killer/T-cell lymphoma: A comparison with conventional staging methods. J Nucl Med 2013;54:1039-44.
[Google Scholar]
|
| 5. |
Yamaguchi M, Kwong YL, Kim WS, Maeda Y, Hashimoto C, Suh C, et al. Phase II study of SMILE chemotherapy for newly diagnosed stage IV, relapsed, or refractory extranodal natural killer (NK)/T-cell lymphoma, nasal type: The NK-Cell Tumor Study Group study. J Clin Oncol 2011;29:4410-6.
[Google Scholar]
|
Fulltext Views
2,821
PDF downloads
3,193





![[Figure - 1]](#fig_ijdvl_2014_80_6_564_144213_u1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2014_80_6_564_144213_u2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2014_80_6_564_144213_u3.jpg){kind=link}