Translate this page into:
Nodular hidradenoma of the scalp: A cytomorphological evaluation on fine needle aspiration cytology
2 Department of Pathology, Pandit Deendayal Upadhyay Government Medical College and Hospital, Rajkot, Gujarat, India
Correspondence Address:
Jitendra G Nasit
C/4, Suryadeep Society, Near Nutan School, Behind Chankyapuri Society, New Sama Road, Vadodara - 390 024, Gujarat
India
| How to cite this article: Nasit JG, Dhruva G. Nodular hidradenoma of the scalp: A cytomorphological evaluation on fine needle aspiration cytology . Indian J Dermatol Venereol Leprol 2014;80:569-572 |
Sir,
Nodular hidradenoma is an uncommon benign adnexal neoplasm of either eccrine or apocrine origin [1],[2],[3] that is commoner in adults than in children. [3],[4] Clinically, it is usually a solitary, slow growing, well circumscribed, freely mobile, firm, non-tender, dermal lesion varying in diameter from 0.5 cm to 12 cm. [1],[3] Occasionally, the development of brown, blue or red discoloration with superficial ulceration and serous discharge may mimic malignancy. [1],[3] Nodular hidradenomas are most commonly seen on the scalp, neck, trunk and extremities. [1],[3],[4] The diagnosis is usually based on histopathology and the lesion is rarely subjected to fine needle aspiration cytology (FNAC). [1],[2],[3],[4],[5],[6],[7],[8]
A 70-year-old male presented with a slowly growing nodule over the scalp for 10 years. Additional complaints of pain, serous discharge and ulceration of skin were present for 1 month. Examination revealed a solitary, non-tender, firm to hard, skin colored swelling of size 3 × 2.5 × 2 cm over the fronto-parietal region of the scalp [Figure - 1]. FNAC was requested without any provisional diagnosis.
 |
| Figure 1: A solitary skin colored nodular swelling measuring 3.0 × 2.5 × 2.0 cm in size on the frontoparietal region of scalp |
Hematoxylin and eosin (H and E) and May-Grόnwald Giemsa (MGG) stained smears showed high cellularity, comprising of numerous large sheets of cells with papillary-like fronds and overcrowded cohesive three-dimensional groups of monomorphic cells. The extracellular eosinophilic hyaline material was intermingled and surrounded by many scattered and loose cohesive cell clusters, resembling rosette-like structures. Occasional duct-like tubular structures were formed by cuboidal cells and filled with hyaline material. Cells were polygonal, containing round to ovoid nuclei with smooth nuclear contour, evenly distributed bland nuclear chromatin, inconspicuous nucleoli and moderate amount of eosinophilic cytoplasm. Some cells showed very scanty cytoplasm, imparting a basaloid appearance. Occasional cells showed clear cytoplasm. A few foam cells were seen in the eosinophilic background [Figure - 2] and [Figure - 3]. The cytologic diagnosis of benign dermal adnexal tumor, not further specified was made.
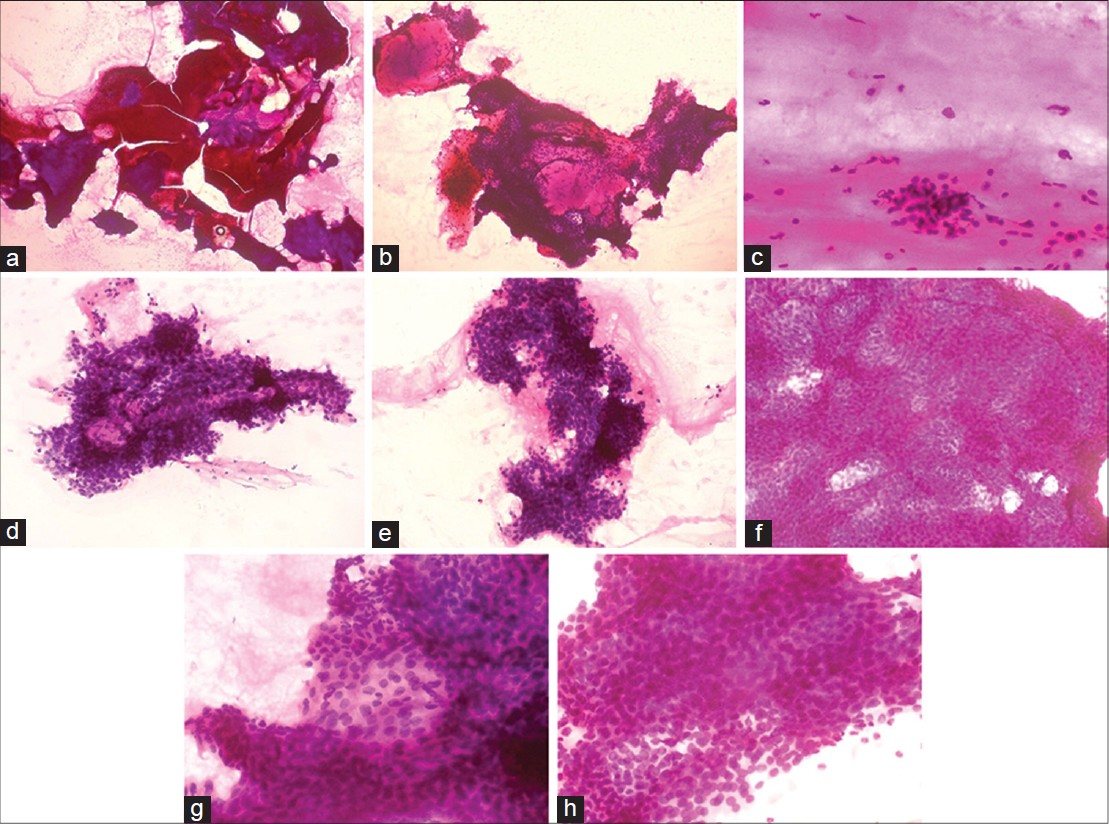 |
| Figure 2: (a) Variabley sized, overcrowded clusters of cells with hyaline material (×40) (b) Eosinophilic hyaline material is surrounded by clusters of cells (×100) (c) Foam cells in fl uidic background (×200) (d) Cuboidal cells forming duct-like tubular structure (×200) (e) Overcrowded papillary-like fronds of polyhedral cells (×200) (f) Large three-dimensional dense sheet of polyhedral cells (×200) (g) Cells show ovoid nuclei, evenly distributed nuclear chromatin, inconspicuous nucleoli and eosinophilic cytoplasm (×400) (h) Scanty cytoplasm of cells, imparting basaloid appearance (H and E×400) |
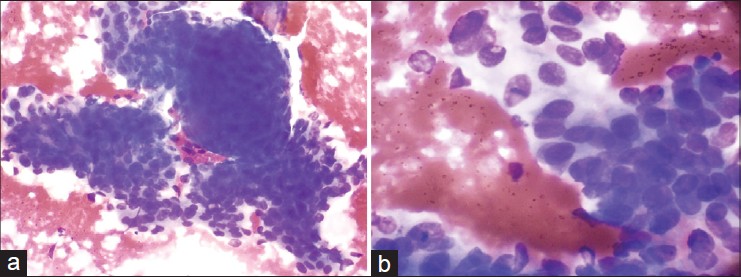 |
| Figure 3: (a) Clusters of overcrowded polygonal cells (×200) (b) Polygonal cells show round to oval bland nucleus and faintly stained cytoplasm. Few cells show clear cytoplasm (×400), May-Grünwald Giemsa stain |
A wide excision with free margins was performed. Histology revealed a well-circumscribed, encapsulated solid-cystic lobulated intradermal tumor. The solid area was composed of two types of cells: eosinophilic/polygonal cells and clear cells. Eosinophilic cells were round to polygonal in shape. They showed a rounded to ovoid nucleus, small distinct nucleoli and faintly eosinophilic cytoplasm. These were also seen to surround hyalinized fibrovascular cores. Clear cells showed abundant clear cytoplasm with a small, round to oval, eccentric nucleus. Some duct-like tubular structures were observed which were constituted by cuboidal cells and filled with eosinophilic hyaline material. Cystic spaces were also filled with amorphous eosinophilic material. Occasional squamoid morules were also evident. Atypia, invasion, necrosis and mitoses were not seen [Figure - 4]. A histologic diagnosis of nodular hidradenoma was made. One year after complete excision, the patient is free of disease.
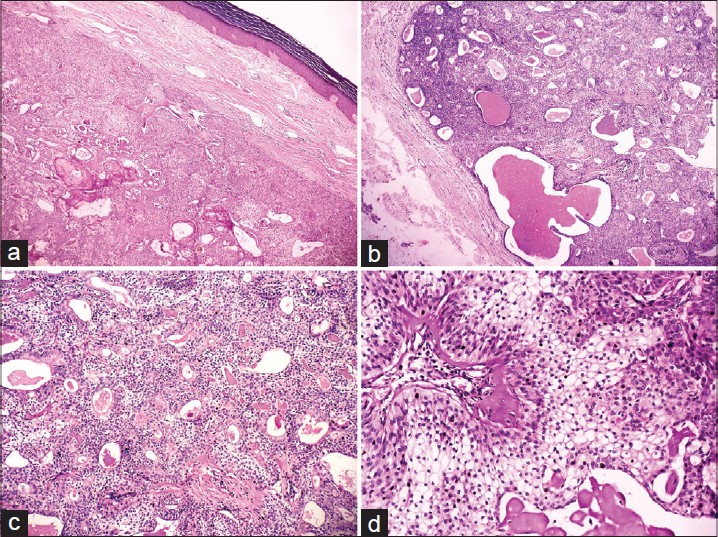 |
| Figure 4: (a) Well-circumscribed encapsulated intradermal tumor shows mainly solid area with few squamoid morules (×40) (b) Dark and lightly stained solid area and amorphous eosinophilic material fi lled cystic spaces (×100) (c) Eosinophilic hyaline material fi lled duct-like tubular structures are formed by cuboidal cells (×200) (d) Hyalinized fibrovascular core surrounded by eosinophilic cells, which show oval nucleus, bland nuclear chromatin, occasional small nucleoli and fi nely granular eosinophilic cytoplasm. Clear cells show abundant clear cytoplasm and small eccentric nucleus (×400), Hematoxylin and eosin (H and E) stain |
Cytological features of nodular hidradenoma are rarely reported in the literature. [3],[8] Most cases of nodular hidradenoma are either inconclusive or misinterpreted on cytology. [1] Smears are usually cellular containing a variable admixture of two types of cells: Eosinophilic/polygonal and clear cells. Eosinophilic cells contain round to ovoid nuclei, small nucleoli and moderate faintly eosinophilic cytoplasm. Occasional cells show scanty cytoplasm with more basaloid appearance while some cells are reminiscent of squamoid cells. Clear cells have round eccentric nuclei, fine granular chromatin, small nucleoli and more abundant, water-clear cytoplasm. Mild hyperchromasia, anisonucleosis and overlapping of nuclei with small distinct nucleoli are also seen. Eosinophilic cells form large, cohesive, three-dimensional papillary-like, densely packed clusters. Clear cells form medium-sized, flat clusters. Rounded rosette-like formations and duct-like tubular structures are also seen. The background shows extracellular hyaline material and amorphous material. Histiocytes, fibrocytes, pigmented macrophages, foam cells and naked nuclei may be seen. [1],[2],[3],[4],[5],[6],[7],[8] The cytology of our case shows all the features reported previously except a prominent clear cell component. Scanty or absent clear cells may be responsible for diagnostic pitfalls. The cytologic appearance of our case closely resembles that of adenoid cystic carcinoma, cutaneous cylindroma and eccrine spiradenoma. Cytology of nodular hidradenocarcinomas shows cells with dense cytoplasm and basaloid appearance, cell sheets with anaplasia and squamous differentiation, necrotic debris and multinucleate giant cells. [9]
Histologically, nodular hidradenoma is a well-circumscribed but unencapsulated solid-cystic dermal tumor with a Grenz zone between the tumor and epidermis. [6] Sometimes it may be encapsulated, as in our case. [1] Cystic spaces may contain eosinophilic homogenous material. Solid areas comprise of eosinophilic/polyhedral and clear cells. Marked nuclear pleomorphism, hyperchromasia and frequent or atypical mitoses are not observed. [1],[3] Variants of nodular hidradenoma may show several types of cells. [3] Clear cell hidradenoma, the most common variant, contains predominantly clear or pale cells with distinct cell borders. Clear cells contain glycogen and periodic acid-Schiff-positive, diastase-resistant material, but no lipid. [3] Poroid hidradenoma shows compact poroid cells with prominent ductal differentiation. [3] Mucinous cells are large cuboidal to columnar in shape with fine basophilic granular cytoplasm and are noted in the least common variant. They line the tubules and may show evidence of apocrine differentiation. [3] As the quantity of different cell types varies markedly in different tumors, cytopathologists and dermatopathologists should be aware of the resemblance of nodular hidradenoma to metastatic renal cell carcinoma, squamous cell carcinoma or signet-ring adenocarcinoma. [3]
To conclude, adequate cellularity on cytology smear is of paramount importance in achieving a specific diagnosis. Cytologically, the finding of two types of cells, eosinophilic and clear cells, three-dimensional clusters with papillary-like fronds, duct-like tubular structures, rosette-like structures and extracellular hyaline material in a cytology smear of a dermal nodule are the key features of nodular hidradenoma.
| 1. |
Grampurohit VU, Dinesh U, Rao R. Nodular hidradenoma of male breast: Cytohistological correlation. J Cytol 2011;28:235-7.
[Google Scholar]
|
| 2. |
Kim YO, Jeon CW, Chang HK. Fine needle aspiration cytology of eccrine acrospiroma of the breast. A report of a case misdiagnosed as ductal carcinoma. Korean J Cytopathol 2005;16:31-5.
[Google Scholar]
|
| 3. |
Novak NP, Kaiæ G, Tomasoviæ-Loncariæ C, Zic R, Skoro M, Ostoviæ KT. Fine-needle aspiration cytology of apocrine hidradenoma. Coll Antropol 2010;34:671-4.
[Google Scholar]
|
| 4. |
Dubb M, Michelow P. Cytologic features of hidradenoma in fine needle aspiration biopsies. Acta Cytol 2009;53:179-82.
[Google Scholar]
|
| 5. |
Agarwal S, Agarwal K, Kathuria P, Jain M, Chauhan DS, Prakash O. Cytomorphological features of nodular hidradenoma highlighting eccrine differentiation: A case report. Indian J Pathol Microbiol 2006;49:411-3.
[Google Scholar]
|
| 6. |
Punia RS, Handa U, Mohan H. Fine needle aspiration cytology of eccrine acrospiroma. Acta Cytol 2001;45:1083-5.
[Google Scholar]
|
| 7. |
Gottschalk-Sabag S, Glick T. Fine-needle aspiration of nodular hidradenoma: A case report. Diagn Cytopathol 1996;15:395-7.
[Google Scholar]
|
| 8. |
Devanand B, Vadiraj P. Fine needle aspiration cytology of eccrine skin adnexal tumors. J Cytol Histol 2011;2:1-7.
[Google Scholar]
|
| 9. |
Garcia-Bonafe MM, Campins MM, Redecilla PH. Malignant nodular hidradenoma on the scalp: Report of a case with fine needle aspiration cytology features and histologic correlation. Acta Cytol 2009;53:576-80.
[Google Scholar]
|
Fulltext Views
6,083
PDF downloads
1,579





![[Figure - 1]](#fig_ijdvl_2014_80_6_569_144218_u1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2014_80_6_569_144218_u2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2014_80_6_569_144218_u3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2014_80_6_569_144218_u4.jpg){kind=link}