Translate this page into:
Non healing solitary noduloulcerative growth over axilla
2 Department of Dermatology, Venereology, and Leprosy, Katihar Medical College, Katihar, Bihar, India
Correspondence Address:
Rajesh Kumar Mandal
Department of Dermatology, Venereology, and Leprosy, North Bengal Medical College, Darjeeling, West Bengal
India
| How to cite this article: Mandal RK, Banerjee S, Koley S, Kumar P. Non healing solitary noduloulcerative growth over axilla. Indian J Dermatol Venereol Leprol 2013;79:112-113 |
Sir,
Basal cell carcinoma (BCC) usually presents on face and other sun exposed parts. Uncommonly, BCC may develop over atypical locations like axilla, nipple, scrotum, pubis, and perianal region posing a diagnostic challenge then. Very few cases of Axillary BCC have been documented in literature and only two cases have been reported from Asia. [1] Here we report a case of axillary BCC due to its extreme rarity and uncommon clinical presentation posing difficulty in diagnosis.
A 45-year-old woman presented with a solitary non-healing, slow growing ulcerative mass in the left axilla for one year [Figure - 1]. The lesion started as small pea sized nodule, which slowly increased in size, and became eroded and ulcerated. There was history of occasional serosanguinous discharge and bleeding from the lesion. There was no history of trauma, radiation, chronic arsenical exposure, and diabetes and no other family member had similar skin lesion. On examination, solitary noduloulcerative growth of 3cm diameter with well-defined fleshy margin was noted in the left axilla. The floor of ulcer showed slough and granulation tissue. Fixity to the underlying tissue and axillary lymphadenopathy were absent. We considered keratoacanthoma, squamous cell carcinoma, donovanosis, and basal cell carcinoma as differential diagnoses. Punch biopsy from the margin of the lesion was taken and sent for histopathology, which revealed epidermal down growths and islands of basaloid cells in dermis [Figure - 2]. The cells were elongated with an elongated oval nucleus and scanty cytoplasm. At the periphery, the cells were arranged in a palisading pattern (fence like) [Figure - 3]. A cleft like space was presented just adjacent to the tumor cell mass at some places. The stroma was loose and fibromyxoid, with scant lymphocytic infiltrate. Based on histopathology findings, we made a diagnosis of BCC and referred the patient to Plastic Surgery Department for excision.
 |
| Figure 1: Noduloulcerative mass over left axilla |
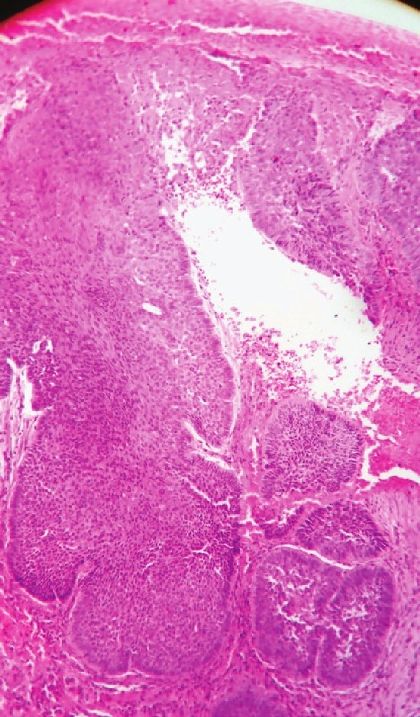 |
| Figure 2: Histology showing down growth of epidermal cells and mass of epidermal cells in the upper dermis (H and E, x100) |
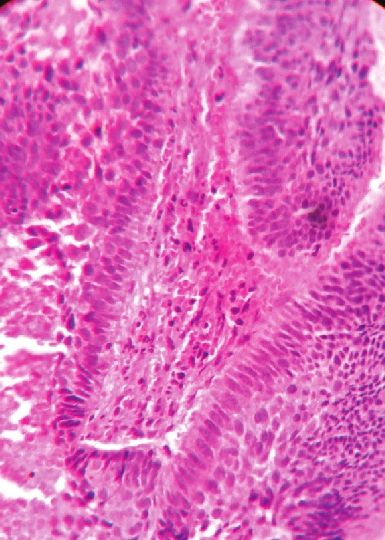 |
| Figure 3: Histology showing mass of basaloid cells with peripheral palisading pattern (H and E, x400) |
BCC is the most common type of cancer in the world which arises from pleuripotent cells within the basal layer of the epidermis or follicular structure, and is mostly seen in fair skinned people over age 40, who are exposed to large amounts of ultraviolet radiation throughout their life. Other known risk factors include chronic exposure to radiation or arsenic, trauma, chronic inflammation, hamartomas, and genetic conditions such as xeroderma pigmentosum and basal cell nevus syndrome.
Noduloulcerative is the most common type of BCC, others being superficial, pigmented, morpheaform and fibroepithelioma of Pinkus. Noduloulcerative BCC is characterized by a pearly/waxy papule with a central depression and overlying telangiectasia. The tumor eventually ulcerates and bleeds, and then, is commonly known as "rodent ulcer". Sunlight exposed skin like head, face and neck is most common site of occurrence but occurrence of BCC over covered sites like nipple, penis, scrotum, vulva, pubis and perianal region have been reported. [2] However, occurrence of BCC in parts, which are usually covered, in persons without any of the above mentioned predisposing factors (as in our case) indicates that etiopathogenesis is still elusive and more studies are needed to identify other contributing factors. One study was done by Zahra Hallaji et al[3] to compare the risk factors associated with single BCC and multiple BCC. They found people born in mountains were at higher risk of developing both single and multiple BCC. This was not reported earlier. Heckmann et al. have proposed "disturbed cell matrix interactions" as a cofactor for developing BCCs. [4] This may explain why some facial areas (such as medial quadrant of the orbit), despite having low Ultraviolet Ray exposure (due to concave shape, reduced skin tension and the presence of marked skin folds), have high frequencies of BCC. Le Sueur et al. proposed that other covered sites might share the same characteristics. [5]
Our case was a noduloulcerative type of BCC but the uncommon location of the lesion and absence of known risk factors (arsenic poisoning, radiation and family history) made the diagnosis challenging. It is not known whether prognosis of a BCC over an uncommon location is any better than those over usual site, but absence of any risk factor is a good prognostic factor. To the best of our knowledge only two cases of axillary BCC were reported from Asia so far and this is the 3 rd case to be reported in Asia. [1] We believe our case to be first case of axillary BCC from India. To conclude, one must keep BCC in mind whenever confronting a noduloulcerative mass, irrespective of the location and history.
| 1. |
Lin CT, Chen SG, Chen TM, Chang SC. Axillary Basal Cell Carcinoma: Case report and literature review. Acta Dermatovenerol Croat 2011;19:107-9.
[Google Scholar]
|
| 2. |
Rahbari H, Mehregan AH. Basal cell epitheliomas in usual and unusual sites. J Cutan Pathol 1979;6:425-31.
[Google Scholar]
|
| 3. |
Hallaji Z, Rahimi H, Mirshams-Shahshahani M. Comparison of risk factors of single basal cell carcinoma with multiple basal cell carcinomas. Indian J Dermatol 2011;56:398-402.
[Google Scholar]
|
| 4. |
Heckmann M, Zogelmeier F, Konz B. Frequency of facial basal cell carcinoma does not correlate with site-specific UV exposure. Arch Dermatol 2002;138:1494-7.
[Google Scholar]
|
| 5. |
LeSueur BW, DiCaudo DJ, Connolly SM. Axillary basal cell carcinoma. Dermatol Surg 2003;29:1105-8.
[Google Scholar]
|
Fulltext Views
2,682
PDF downloads
1,622





![[Figure - 1]](#fig_ijdvl_2013_79_1_112_104684_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2013_79_1_112_104684_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2013_79_1_112_104684_f3.jpg){kind=link}