Translate this page into:
Painful nodule on forearm
2 National institute of pathology (Indian council of medical research), Safdarjung Hospital, New Delhi, India
Correspondence Address:
Jyoti Gupta
W-5, Green Park, New Delhi - 110 016
India
| How to cite this article: Gupta J, Paliwal P, Ramesh V. Painful nodule on forearm. Indian J Dermatol Venereol Leprol 2013;79:551-552 |
An 8-year-old boy presented with complaints of progressively increasing, painful, swelling on left wrist present since birth. On examination, a 2 cm × 3 cm, soft, tender, ill-defined, skin colored nodule, with lobulated surface, better felt than seen was present over the flexor aspect of left wrist [Figure - 1]. Neither hypertrichosis nor noticeable perspiration was present. A 4 mm punch biopsy revealed a normal to acanthotic epidermis with dermal proliferation of well-differentiated eccrine glands, in close association with a few well-differentiated, thin-walled angiomatous channels ,and adipose tissue [Figure - 2]. Nerve fibers were noted adjoining vascular channels in a majority of the eccrine units [Figure - 3]. No atypia or mitosis was noted.
 |
| Figure 1: Skin colored nodule over wrist with biopsy mark on left side of the lesion |
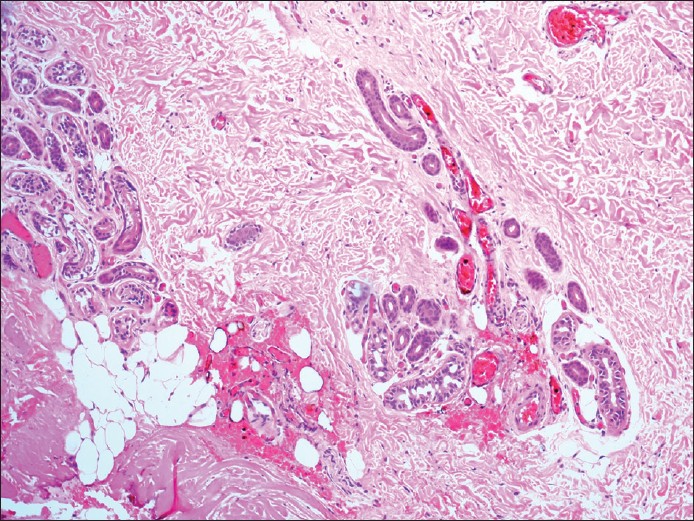 |
| Figure 2: Dermal proliferation of eccrine glands along with thin-walled vascular channels and adipose tissue (H and E, × 40) |
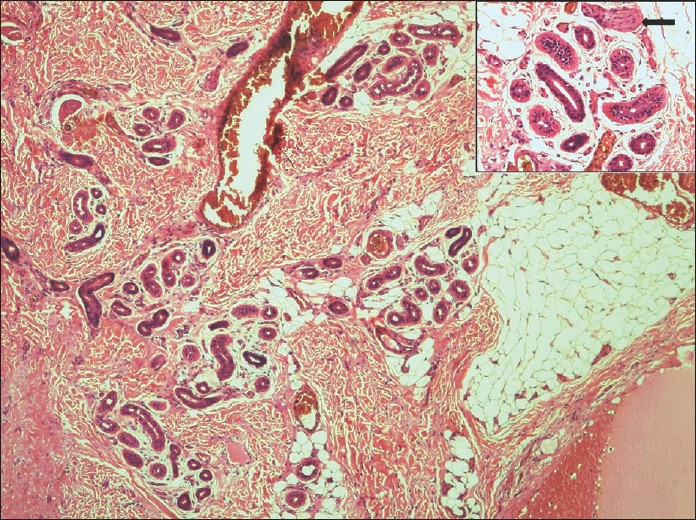 |
| Figure 3: Dermal proliferation of eccrine glands along with thin-walled vascular channels and adipose tissue (H and E, × 100). Inset showing nerve fiber adjoining vascular channels (H and E, × 400) |
What is your diagnosis?
Answer: Eccrine angiomatous hamartoma (EAH)
EAH is a rare, benign vascular malformation that usually presents at birth, early childhood or rarely adulthood [1] without a gender predilection. Clinically, it presents as a nodule or a plaque, usually solitary, mostly located on the extremities (80%), however, other locations like trunk, neck, face, and vulva have been reported. The lesions are generally asymptomatic, however, focal hyperhidrosis, hypertrichosis, and pain can be observed. [2] Infiltration of nerves among the eccrine glands may be responsible for the pain. [3] Rapid growth may occur during puberty and pregnancy, suggesting underlying hormonal influence. [4]
Histopathological examination reveals an increase in number of thin walled vascular channels in addition to increase in eccrine glands. Other variants with increased dermal mucin, and the presence of hair follicles or nerve fibers have been described. [2] Verrucous change in overlying epidermis has been reported. Immunohistochemistry shows diminished levels of carcino embryonic antigen and S-100 protein, which are commonly found in the eccrine sweat apparatus. [4]
Clinically, differential diagnosis may include eccrine nevus, tufted angioma, glomus tumor, smooth muscle hamartoma, sudoriparous angioma, and angioleiomyoma. Histopathological overlap occurs in sudoriparous angioma and eccrine nevus while others are distinct histological entities. In sudoriparous angioma, the angiomatous component predominates, and the eccrine glands show dilatation instead of proliferation. [2] Eccrine nevus is composed of mature eccrine glands without angiomatous proliferation. [2]
EAH is a benign tumor and does not require aggressive treatment when asymptomatic. Spontaneous regression may occur. Simple excision is usually curative and is reserved for symptomatic cases or for cosmetic reasons. Recurrences have been rarely reported. [5] In our patient, simple excision was carried out as the lesion was painful. The excision proved to be curative, and patient is asymptomatic after 3 months of follow-up.
| 1. |
Natarajan K, Rai R, Sundararajan V, Venkatchala S. Eccrine angiomatous hamartoma in an adult. Indian J Dermatol Venereol Leprol 2009;75:193-4.
[Google Scholar]
|
| 2. |
Foshee JB, Grau RH, Adelson DM, Crowson N. Eccrine angiomatous hamartoma in an infant. Pediatr Dermatol 2006;23:365-8.
[Google Scholar]
|
| 3. |
Wolf R, Krakowski A, Dorfman B, Baratz M. Eccrine angiomatous hamartoma. A painful step. Arch Dermatol 1989;125:1489-90.
[Google Scholar]
|
| 4. |
Sulica RL, Kao GF, Sulica VI, Penneys NS. Eccrine angiomatous hamartoma (nevus): Immunohistochemical findings and review of the literature. J Cutan Pathol 1994;21:71-5.
[Google Scholar]
|
| 5. |
Sen S, Chatterjee G, Mitra PK, Gangopadhyay A. Eccrine angiomatous naevus revisited. Indian J Dermatol 2012;57:313-5.
[Google Scholar]
|
Fulltext Views
2,398
PDF downloads
1,341





![[Figure - 1]](#fig_ijdvl_2013_79_4_551_113105_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2013_79_4_551_113105_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2013_79_4_551_113105_f3.jpg){kind=link}