
Translate this page into:
Paradoxical psoriasis induced by IL-17 antagonists
Corresponding author: Dr. Suju Luo, Department of Dermatology, Tianjin Medical University General Hospital, Anshan Dao, Tianjin, China. luosuju@tmu.edu.cn
-
Received: ,
Accepted: ,
How to cite this article: Wang Y, Yang F, Wang R, Luo S. Paradoxical psoriasis induced by IL-17 antagonists. Indian J Dermatol Venereol Leprol. doi: 10.25259/IJDVL_719_2023
Abstract
Background
The paradoxical occurrence of psoriasis triggered by Interleukin-17 (IL-17) inhibitors is notable due to its prominent symptoms and the therapeutic dilemma it presents for follow-up care.
Objective
To describe cases in our clinic, perform an in-depth literature review, and suggest the most probable mechanisms of action.
Method
We conducted a literature review on published cases of IL-17 inhibitor-induced psoriasis.
Results
We found 22 articles reporting 30 cases of IL-17 inhibitor-induced paradoxical psoriasis, primarily observed in patients with a previous psoriasis history. Almost 60% of cases showed a change in lesion morphology, with the plaque or pustular type being prevalent. About 73.3% of patients had to discontinue the implicated drug, leading to partial or complete symptom resolution. The mechanism behind this response seemed to involve IL-17 inhibitors downregulating Tumour Necrosis Factor alpha (TNF-α), subsequently upregulating plasmacytoid dendritic cells and triggering unopposed IFN-alpha (IFN-α) production.
Limitation
Data are confined to case reports and case series.
Conclusion
More assertive measures are recommended for treating paradoxical psoriasis induced by IL-17 inhibitors than those caused by TNF-α inhibitors. Reintroducing an IL-17 inhibitor is not advised, as patients did not show improvement.
Keywords
IL-17 inhibitor
paradoxical eruption
paradoxical psoriasis
psoriasis
pathogenesis

Introduction
The three approved IL-17 inhibitors consist of IL-17A inhibitors (secukinumab and ixekizumab) and an IL-17 receptor (IL-17R) inhibitor (brodalumab). They exhibit satisfactory therapeutic outcomes and acceptable safety profiles in treating psoriasis and psoriatic arthritis. However, occasional reports highlight less common side effects during anti-IL-17 treatment, such as paradoxical reactions. These reactions are notable for their unmistakable symptoms and the subsequent therapeutic challenge in follow-up care. Paradoxical reactions are generally defined as developing or worsening a preexisting immune-mediated disorder that would typically respond to the same therapeutic agent causing it.1 In this context, we present a case series of patients who developed paradoxical psoriasis during anti-IL-17 treatment at our institution. We also review relevant articles, aiming to propose the most likely mechanisms of action and a relatively optimised therapeutic approach for physicians to consider as a reference.
Materials and Methods
We conducted a literature review using the PubMed and MEDLINE databases (updated through January 1, 2023). The search employed index terms like “anti-interleukin 17,” “ixekizumab,” “secukinumab,” and “brodalumab,” combined,” coupled with terms such as “paradoxical,” “psoriasis,” “arthritis,” “skin,” and “eruption.” Additionally, we reviewed citations within the articles to ensure comprehensive coverage. Patients with other established trigger factors were excluded from this review. Moreover, we present a case series of patients with preexisting psoriasis who developed paradoxical psoriasis eruptions during anti-IL-17 treatment in our institution from June 2020 to August 2022. All patients provided written informed consent, and the ethics committee approved the study.
Case Series
Case 1: A 59-year-old man had plaque psoriasis for over 30 years, along with type 2 diabetes and coronary artery disease for 10 years. And he was referred to our clinic, due to a sudden bout of erythroderma (Body surface area, BSA = 92%; Psoriasis area severity index, PASI = 65) [Figure 1a]. His medical history revealed regular use of Chinese herbal medicines for psoriasis, and he had been on hypoglycemic drugs and antihypertensives for a long time to manage his other health issues. Consequently, ixekizumab treatment was initiated at the prescribed dosages. Ten days later, PASI decreased to 29.2 [Figure 1b]. Unfortunately, the positive response halted in the 3rd week, and erythroderma returned in the first month of ixekizumab treatment (PASI = 64.8) [Figure 1c]. No specific factors were identified as the cause for this deterioration. Due to the worsening of the disease, ixekizumab was stopped, and acitretin combined with cyclosporine was started to improve the condition. After 6 days of this treatment, erythema and edema showed significant improvement, and simultaneously, PASI decreased to 45 [Figure 1d].

- Erythrodermic psoriasis was diagonsed at the initial visit in case 1.

- After 10 days of treatment with ixekizumab in case 1.

- Paradoxical psoriasis was diagnosed after 1 month of treatment with ixekizumab in case 1
- After discontinuation of ixekizumab and treatment with acitretin and cyclosporine for 6 days in case 1.
Case 2: An 18-year-old woman, having psoriasis vulgaris for 8 years, was referred to our clinic due to erythroderma and psoriatic arthritis [Figure 2a]. A physical examination showed widespread redness and rough scaly plaques covering nearly all skin (BSA = 98%; PASI = 56.4). After a thorough assessment, ixekizumab was initiated. PASI decreased to 25.6 entirely following the second dose, and troublesome joint symptoms significantly improved [Figure 2b]. However, this positive response lasted for only one more week. During the 6-week follow-up, erythroderma reappeared without apparent cause (PASI = 62.4) [Figure 2c]. Consequently, ixekizumab was discontinued, and adalimumab was started. In another 3-month follow-up, the rash was nearly cleared (PASI = 2) [Figure 2d].

- Erythrodermic psoriasis was diagnosed at the initial visit in case 2.
- After 14 days of treatment with ixekizumab in case 2.

- Paradoxical psoriasis was diagnosed after six weeks of treatment with ixekizumab in case 2.
- After discontinuation of ixekizumab and treatment with adalimumab for 5 weeks in case 2.
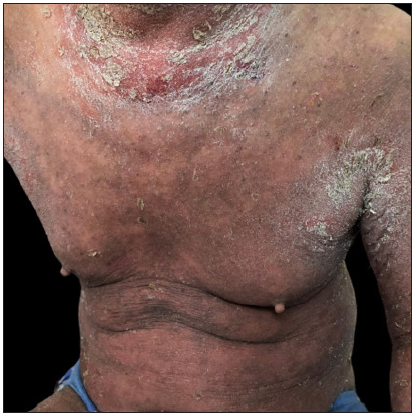
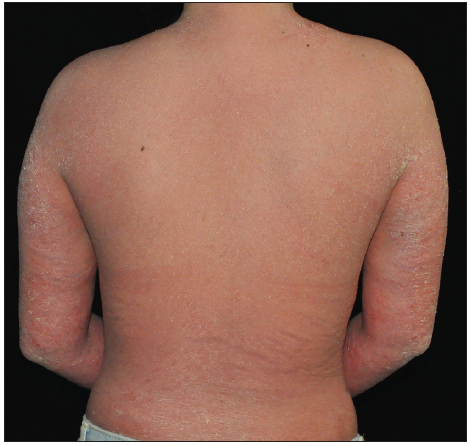
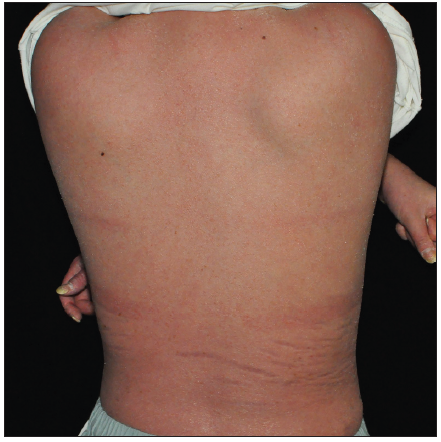
Case 3: A 19-year-old overweight man, diagnosed with plaque psoriasis for 8 years and recently found to have metabolic syndrome, was referred to our clinic due to the significant impact of the disease on his quality of life [Figure 3a]. Previous medical records indicated a refusal of traditional systemic agents due to potential adverse effects. A physical examination revealed widespread redness and thickened scaly plaques covering the skin (BSA = 70%, PASI = 40.8). Consequently, ixekizumab was administered at the recommended dosages. By the 2nd week, PASI decreased to 19.6 [Figure 3b]. However, by the 5th week, guttate psoriasiform eruptions appeared on the ventral and dorsal trunk, and the bilateral lower limbs were covered with coarse plaques without any identifiable triggers (PASI = 29.7) [Figure 3c]. To address this, topical corticosteroids were added for rescue, but the outcomes were unsatisfactory. Subsequently, ixekizumab was stopped, and adalimumab was initiated. Unfortunately, at the 3-month follow-up, the eruption had only partially improved (PASI = 20.7) [Figure 3d].

- Plaque psoriasis was diagnosed at the initial visit in case 3.
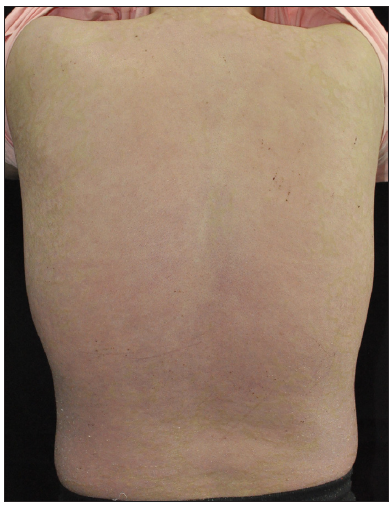
- After 14 days of treatment with ixekizumab in case 3.
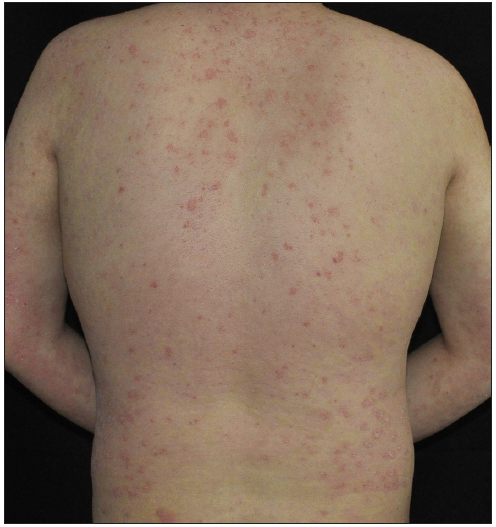
- Paradoxical psoriasis was diagnosed after 5 weeks of treatment with ixekizumab in case 3.

- After discontinuation of ixekizumab and treatment with adalimumab for 3 months in case 3.
Case 4: A 24-year-old woman, diagnosed with plaque psoriasis for 8 years, was referred to our clinic [Figure 4a]. No prior medical history was available. A physical examination showed generalised thick scaly plaques (BSA = 30%, PASI = 24.3). Ixekizumab was then prescribed. Within 2 weeks, the PASI decreased to 11.1 [Figure 4b]. Unfortunately, by the 3rd week, annular lesions developed and spread on the trunk and gradually onto the limbs despite the application of potent topical corticosteroids (PASI = 29.7) [Figure 4c]. No specific triggers were identified during this time. Consequently, we switched from ixekizumab to adalimumab in the 5th week. At the 3-month follow-up, the lesions were almost resolved (PASI = 0.6) [Figure 4d].

- After 14 days of treatment with ixekizumab in case 4.

- Plaque psoriasis was diagnosed at the initial visit in case 4.

- Paradoxical psoriasis was diagnosed after 5 weeks of treatment with ixekizumab in case 4.

- After discontinuation of ixekizumab and treatment with adalimumab for 3 weeks in case 4.
Results
A total of 22 articles, including 30 patients, were included in the final analysis. Gender, age, comorbidities, diagnosis, drug administration, the progression of skin eruption, and management details are presented in Tables 1 and 2. As indicated in Table 1, the onset time of paradoxical psoriasis varied, ranging from 1 week to 2 years. Preexisting psoriasis deteriorated in most cases (except for three patients with different major diagnoses). Conversion of lesion morphology during anti-IL-17 therapy was observed in 59.3% (16/27) of patients, with 3 cases developing de novo psoriasis. Among these, the conversion of plaque to pustular was the most common, accounting for approximately 68.8% (11/16).
| Total (n = 30) | PSO (n = 27) | AS (n = 2) | HS (n = 1) | |
|---|---|---|---|---|
| Male | 14 (46.6) | 14 (51.9) | N | N |
| Female | 16 (53.3) | 13 (48.1) | 2 (100) | 1 (100) |
| Age, mean ± SD years | 49.7 ± 12.7 | 49.8 ± 13.0 | 55.5 ± 2.1 | 36.0 |
| Culprit drug | ||||
| Ixekizumab | 9 (30.0) | 9 (33.3) | N | N |
| Secukinumab | 14 (46.6) | 11 (40.7) | 1 (100) | 1 (100) |
| Brodalumab | 7 (23.3) | 7 (25.9) | N | N |
| Types of new onset or exacerbation psoriasis | ||||
| Guttate | 1 (3.3) | 1 (3.7) | N | N |
| Plaque | 10 (33.3) | 10 (37.0) | 1 (50) | N |
| Pustular | 11 (36.6) | 9 (33.3) | 1 (50) | 1 (100) |
| Arthritis | 3 (10.0) | 3 (11.1) | N | N |
| Erythroderma | 1 (3.3) | 1 (3.7) | N | N |
| Mixed | 4 (13.3) | 4 (14.8) | N | N |
| Latent period, mean ± SD weeks | 23.0 ± 21.4 | 23.2 ± 21.9 | 24.0 ± 28.2 | 16.0 |
| Management | ||||
| Continuation of anti-IL-17 without adjuvant therapy | N | N | N | N |
| Continuation of anti-IL-17 with topical therapy | 6 (20.0) | 6 (22.2) | N | N |
| Continuation of anti-IL-17 with systemic therapy | 2 (6.6) | 2 (9.1) | N | N |
| Withdrawn anti-IL-17 without adjuvant therapy | N | N | N | N |
| Withdrawn anti-IL-17 with topical therapy | 6 (20.0) | 3 (11.1) | 2 (100) | 1 (100) |
| Withdrawn anti-IL-17 with systemic therapy | 16 (53.3) | 16 (59.3) | N | N |
| Outcome | ||||
| Partial or complete resolution | 28 (93.3) | 25 (92.6) | 2 | 1 |
| No resolution | 2 (6.6) | 2 (7.4) | N | N |
Values are the number (percentage) unless otherwise indicated. N: none; PSO: psoriasis; AS: ankylosing spondylitis; HS: hidradenitis suppurativa SD: standard deviation.
| Number | Reference | Sex/age (years) | Diagnose | Comorbidity | Anti-IL-17 agent | Time to onset or exacerbation of psoriasis (weeks) | Conversion of lesion morphology during anti- IL-17 therapy | Management | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Hoshina et al.4 | F/43 | PSO | PSA | Secukinumab | 4 | Plaque to plaque | Secukinumab discontinuation+systemic CsA | Gradually improved |
| 2 | Pirro et al.5 | M/48 | PSO | N | Ixekizumab | 16 | Plaque to pustular | Ixekizumab maintenance+topical steroids | Completely resolved |
| 3 | Vidal et al6 | M/46 | PSO | N | Ixekizumab | 2 | Plaque to arthritis | Ixekizumab discontinuation+ Secukinumab + short-term systemic steroids | Completely resolved |
| 4 | Martínez-Doménech et al.7 | M/43 | PSO | N | Ixekizumab | 48 | Pustular to Pustular | Ixekizumab maintenance + topical steroids | No resolution |
| 5 | Oiwa et al.8 | M/76 | PSO | N | Ixekizumab | 8 | Plaque to erythroderma | Ixekizumab discontinuation + systemic CsA | Mostly resolved |
| 6 | Cicogna et al.9 | F/52 | PSO | PSA | Secukinumab | 36 | Plaque to pustular | Secukinumab discontinuation + systemic acitretin | Visibly regressed |
| 7 | Caldarola et al.10 | M/34 | PSO | N | Ixekizumab | 8 | Plaque to plaque | Ixekizumab maintenance + topical steroids | Improved |
| 8 | Caldarola et al.10 | M/53 | PSO | N | Ixekizumab | 20 | Plaque to plaque | Ixekizumab discontinuation + topical steroids | Improved |
| 9 | Caldarola et al.10 | M/52 | PSO | N | Secukinumab | 16 | Plaque to plaque | Secukinumab discontinuation + topical steroids | Improved |
| 10 | Caldarola et al.10 | M/48 | PSO | N | Ixekizumab | 12 | Plaque to plaque | Ixekizumab maintenance + topical steroids | Improved |
| 11 | Caldarola et al.10 | F/42 | PSO | N | Ixekizumab | 26 | Plaque to plaque | Ixekizumab maintenance + topical steroids | Improved |
| 12 | Tan et al.11 | F/62 | PSO | Hypertension, diabetes, and essential tremor | Ixekizumab | 24 | Plaque to plaque | Ixekizumab discontinuation + short-term systemic steroids | Mild improved |
| 13 | Takahashi et al.12 | F/69 | PSO | N | Brodalumb | 16 | Plaque to pustular with PSA | Brodalumb discontinuation + systemic CsA | Rapidly improved |
| 14 | Takahashi et al.12 | M/63 | PSO | N | Brodalumb | 12 | Plaque to arthritis | Brodalumb discontinuation + adalimumab | Rapidly improved |
| 15 | Sadik et al.13 | F/42 | PSO | N | Brodalumb | 24 | Plaque to pustular with PSA | Brodalumb discontinuation + ustekinumab | Gradually resolved |
| 16 | Kurtipek et al.14 | M/33 | PSO | N | Secukinumab | 20 | Plaque to guttate | Secukinumab maintenance + short-term MTX | No regression |
| 17 | Honma et al.15 | F/64 | PSO | N | Secukinumab | 96 | Pustular to Pustular | Secukinumab maintenance+ topical steroids | No worsening |
| 18 | Abbruzzese et al.16 | F/63 | PSO | PSA | Secukinumab | 36 | Plaque to pustular | Secukinumab maintenance + systemic CsA | Completely resolved |
| 19 | Currado et al.17 | F/54 | AS | N | Secukinumab | 44 | New onset plaque | Secukinumab discontinuation + topical agents | Completely resolved |
| 20 | Sladden et al.18 | F/61 | PSO | N | Secukinumab | 12 | Plaque to pustular | Secukinumab discontinuation+ ustekinumab | Significantly improved |
| 21 | Noell et al.19 | M/53 | PSO | N | Secukinumab | 5 | Plaque to plaque | Secukinumab discontinuation + infliximab | Promising improved |
| 22 | Dogra et al.20 | M/22 | PSO | N | Secukinumab | 36 | Plaque to pustular | Secukinumab discontinuation + Infliximab | Completely resolved |
| 23 | Mössner et al.21 | F/26 | PSO | N | Brodalumb | 8 | Plaque to pustular | Brodalumb discontinuation + ustekinumab | Completely resolved |
| 24 | Mössner et al.21 | F/44 | PSO | PSA and obesity | Secukinumab | 64 | Plaque to pustular | Secukinumab discontinuation + topical steroids | Completely resolved |
| 25 | Mössner et al.21 | F/45 | PSO | PSA and obesity | Secukinumab | 56 | Plaque to pustular with plaque | Secukinumab discontinuation + ustekinumab | considerably improved |
| 26 | Penalba-Torres et al.22 | F/36 | HS | N | Secukinumab | 16 | New onset pustular | Secukinumab discontinuation + topical agents | Completely resolved |
| 27 | Penalba-Torres et al.22 | F/57 | AS | N | Secukinumab | 4 | New onset pustular | Secukinumab discontinuation + topical agents | Rapidly improved |
| 28 | Hosokawa et al.23 | M/67 | PSO | N | Brodalumb | 4 | Plaque to plaque | Brodalumb discontinuation + Guselkumab | Visibly improved |
| 29 | Kashlan et al.24 | M/47 | PSO | PSA and obesity | Brodalumb | 1 | Plaque to recurred arthritis | Brodalumb discontinuation + to facitinib + short-term systemic steroids | Improved |
| 30 | Caravello et al.25 | M/46 | PSO | N | Brodalumb | 16 | Plaque to pustular with plaque | Brodalumb discontinuation + Secukinumab | Partial improved |
Abbreviation: F: female; M: male; N: none; PSO: psoriasis; PSA: psoriatic arthritis; HS: hidradenitis suppurativa; AS: ankylosing spondylitis; CsA: Cyclosporin.
The management of paradoxical psoriasis varied widely due to patient heterogeneity. Among the 30 patients, 53.3% switched to another systemic agent, 20% suspended the culprit drug and added topical agents, 20% added topical agents without discontinuing the drug, and 6.6% continued the drug with another systemic agent as a complement. In the follow-up, 93.3% of cases showed partial or complete resolution, regardless of drug continuation, while 6.6% exhibited no resolution, primarily in patients maintaining the culprit drug. Interestingly, two cases reintroduced a different class of IL-17 inhibitors for treating paradoxical psoriasiform eruptions, with no observed deterioration and partial improvement of the disease. Additionally, 71.4% (5/7) of patients with comorbidities discontinued the original drug and switched to another systemic agent. For patients without comorbidities, 47.8% (11/23) made the same decision for management. Subgroup analysis generally mirrored the overall group analysis.
Discussion
IL-17A/IL-17R inhibitors are effective and safe in large-scale randomised controlled trials for treating psoriasis and psoriatic arthritis. However, occasional reports of less common side effects, such as paradoxical psoriasis, have emerged. This paper presents representative cases of paradoxical psoriasis induced by IL-17A inhibitors in our institution. Our findings suggest that our patients may be more susceptible to severe attacks with a shorter latency compared to previous studies. Although three out of four patients had comorbidities [Table 3], and one had experienced multiple agents, we attribute the sudden deterioration to paradoxical psoriasis rather than the above mentioned factors. A multicenter retrospective study revealed that ixekizumab response was unaffected by clinical variables like body mass index, disease duration, or psoriatic arthritis, further supporting our opinion.2
| Patient | Sex/age (years) | Diagnose | Comorbidity | PASI (start) | PASI (remission) | PASI (exacerbation) | PASI (at the last follow-up) | Time to exacerbation of psoriasis (weeks) | Conversion of lesion morphology | Management |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M/59 | EP | Type 2 diabetes; cardiovascular diseases | 65 | 29.2 | 64.8 | 45 | 3 | No change | Acitretin combined with CsA + ixekizumab discontinuation. |
| 2 | F/18 | EP | PSA | 56.4 | 25.6 | 62.4 | 2 | 3 | No change | Adalimumab + ixekizumab discontinuation |
| 3 | M/19 | PP | Metabolic syndrome | 40.8 | 19.6 | 29.7 | 20.7 | 5 | Plaque to guttate | Adalimumab + ixekizumab discontinuation |
| 4 | F/24 | PP | N | 24.3 | 11.1 | 29.7 | 0.6 | 3 | No change | Adalimumab + ixekizumab discontinuation |
Abbreviation: F: female; M: male; N: none; PP: plaque psoriasis; PSA: psoriatic arthritis; EP: erythroderma psoriasis; CsA: cyclosporin; PASI: psoriasis area severity index.
Reviewing the literature on IL-17 inhibitor-induced paradoxical psoriasis; we observed that compared with TNF-α inhibitors, the latency was shorter, and the lesion morphology tended to transform plaque into pustular rather than plaque to guttate. Mechanistically, IL-17 inhibitors lead to a decrease in TNF-α concentrations, directly or indirectly causing an increase in IFN-α. This, in turn, leads to the expression of chemokines such as CXCR3 on T cells, promoting T-cell homing to the skin and sustaining the inflammatory mechanisms of psoriasis lesions.3 Inhibition of Th17 may cause repolarization toward Th1, possibly explaining why TNF-α inhibitors can manage paradoxical psoriasis caused by IL-17 inhibitors.
There is no consensus on managing paradoxical psoriasis induced by IL-17 inhibitors due to limited reported data.4–25 In our study, we found that more patients preferred discontinuing the implicated drug and sought additional adjuvant therapy to control paradoxical psoriasis, in contrast to that induced by TNF-α inhibitors (73.3% vs. 33.2%). Patients attempting to continue IL-17 inhibitors without strong intervention faced more significant challenges instead of gradual improvement. This evidence suggests that more aggressive measures should be taken to treat paradoxical psoriasis induced by IL-17 inhibitors than those caused by TNF-α inhibitors. Reintroducing another IL-17 inhibitor is not recommended, as patients rarely improved according to this analysis.
Limitation
Data are limited to case reports and case series.
Conclusion
A substantial body of evidence suggests that patients in similar situations may benefit from more aggressive interventions. Additionally, the re-administration of another IL-17 inhibitor is not recommended.
Ethical approval
This study was approved by the Ethics Committee of Tianjin Medical University General Hospital, Tianjin Medical University (IRB2022-WZ-066).
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
National Natural Science Foundation of China (Grant No. 81773319).
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Autoimmune diseases induced by biological agents: A double-edged sword? Autoimmun Rev. 2010;9:188-93.
- [CrossRef] [PubMed] [Google Scholar]
- Initial results of ixekizumab efficacy and safety in real-world plaque psoriasis patients: A multicentre retrospective study. J Eur Acad Dermatol Venereol. 2019;33:553-9.
- [CrossRef] [PubMed] [Google Scholar]
- Paradoxical reactions under TNF-α blocking agents and other biological agents for chronic immune-mediated diseases: An analytical and comprehensive overview. RMD Open. 2016;2:e000239.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Paradoxical localized exacerbation of psoriatic eruptions triggered by secukinumab. Clin Exp Dermatol. 2018;43:718-19.
- [CrossRef] [PubMed] [Google Scholar]
- Multiple paradoxical reactions during ixekizumab therapy. Dermatol Ther. 2019;32:e12852.
- [CrossRef] [PubMed] [Google Scholar]
- Paradoxical arthritis due to ixekizumab in a patient with plaque psoriasis. Actas Dermosifiliogr. 2019;110:255-6.
- [CrossRef] [PubMed] [Google Scholar]
- Paradoxical reversed plantar involvement during ixekizumab therapy for psoriasis. Dermatol Online J. 2019;25:13030/qt4624n3hj.
- [PubMed] [Google Scholar]
- A case of ixekizumab-induced psoriasiform eruption. Acta Derm Venereol. 2019;99:446-7.
- [CrossRef] [PubMed] [Google Scholar]
- Case report: Paradoxical acrodermatitis of Hallopeau-like eruption following anti-IL-17 therapy. F1000Res. 2019;8:336.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Clinical and histopathological characterization of eczematous eruptions occurring in course of anti IL-17 treatment: A case series and review of the literature. Expert Opin Biol Ther. 2020;20:665-72.
- [CrossRef] [PubMed] [Google Scholar]
- Drug-induced psoriasiform alopecia associated with interleukin-17 inhibitor therapy. J Cutan Pathol. 2021;48:771-4.
- [CrossRef] [PubMed] [Google Scholar]
- Brodalumab-induced palmar pustular eruption and joint swelling accompanied by muscle pains in two cases of psoriasis. J Dermatol. 2018;45:e325-6.
- [CrossRef] [PubMed] [Google Scholar]
- First emergence of pyoderma gangraenosum, palmoplantar pustulosis and sacroiliitis in a psoriasis patient associated with switching from secukinumab to brodalumab. J Eur Acad Dermatol Venereol. 2019;33:e406-7.
- [CrossRef] [PubMed] [Google Scholar]
- Unusual relapse in a psoriasis patient receiving secukinumab: Linear psoriasis. Dermatol Ther. 2020;33:e13346.
- [CrossRef] [PubMed] [Google Scholar]
- Palmoplantar pustulosis emerged on a case of generalized pustular psoriasis successfully treated by secukinumab. J Dermatol. 2019;46:e468-9.
- [CrossRef] [PubMed] [Google Scholar]
- Paradoxical pustular psoriasis in a patient with psoriatic arthritis on secukinumab treatment. J Clin Rheumatol. 2020;26:e208-9.
- [CrossRef] [PubMed] [Google Scholar]
- New onset of psoriasis induced by secukinumab in a patient with ankylosing spondylitis: A case report. Scand J Rheumatol. 2020;49:75-6.
- [CrossRef] [PubMed] [Google Scholar]
- Secukinumab-induced psoriasiform eruption. JAMA Dermatol. 2017;153:1194-5.
- [CrossRef] [PubMed] [Google Scholar]
- Anti IL-17 flared psoriasis in a patient on secukinumab. Dermatol Ther 2017
- [CrossRef] [PubMed] [Google Scholar]
- Secukinumab-induced paradoxical pustular psoriasis. Clin Exp Dermatol. 2019;44:72-3.
- [CrossRef] [PubMed] [Google Scholar]
- Paradoxical palmoplantar pustulosis induced by secukinumab and brodalumab: A report of three cases. Eur J Dermatol. 2020;30:177-209.
- [CrossRef] [PubMed] [Google Scholar]
- Palmoplantar pustulosis under secukinumab in two patients without psoriasis. J Dtsch Dermatol Ges. 2022;20:106-9.
- [CrossRef] [PubMed] [Google Scholar]
- Effective treatment with guselkumab for psoriatic alopecia as paradoxical reaction. J Dermatol. 2019;46:e302-3.
- [CrossRef] [PubMed] [Google Scholar]
- Paradoxical psoriatic arthritis flare with the initiation of brodalumab and guselkumab. JAAD Case Rep. 2021;10:47-9.
- [CrossRef] [PubMed] [Google Scholar]
- Paradoxical reaction to brodalumab in a patient affected by psoriasis. Ital J Dermatol Venerol. 2021;156:511-2.
- [CrossRef] [PubMed] [Google Scholar]




