
Translate this page into:
Partial unilateral lentiginosis with ipsilateral Lisch nodules and pilocytic astrocytoma: Is this a type of segmental neurofibromatosis?
Corresponding author: Dr. Yasemin Erdem, Department of Dermatology, Health Science University Sisli Hamidiye Etfal Training and Research Hospital, Sisli, Istanbul, Turkey. erdemyasemin1@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Erdem Y, Altunay IK, Ozkur E, Duzgun E. Partial unilateral lentiginosis with ipsilateral lisch nodules and pilocytic astrocytoma: Is this a type of segmental neurofibromatosis? Indian J Dermatol Venereol Leprol 2021;87:109-111.
Sir,
Partial unilateral lentiginosis, also termed as segmental lentiginosis, is a rare pigmentation disorder characterized by numerous lentigines on normal skin. Since Lisch nodules, cafe au-lait macules and axillary freckling may accompany partial unilateral lentiginosis, the disorder has been accepted as a form of segmental neurofibromatosis by some authors in recent years.1,2 Herein, we report a case of partial unilateral lentiginosis which is accompanied by ipsilateral Lisch nodules and pilocytic astrocytoma.
A 28-year-old woman with spotty lesions on the face and body was referred to us from the neurosurgery department. She underwent surgery in the past year for pilocytic astrocytoma at the level of the 2nd cervical vertebra, and she has been under follow-up at the neurosurgery polyclinic [Figure 1]. Dermatologic examination of the patient revealed sharply circumscribed, multiple dark brown macular lesions with 2–3 mm size on a light brown background. These lesions were located at the right side of the face, at the right scapular area in conjunction with the right arm and on the medial side of the right leg [Figures 2a, 2b and 2c]. None of the lesions extended beyond the midline. These lesions occurred 1 year ago, and no change was observed in the color, and dimensions of the lesions during this period. No cafe au-lait macules, axillary freckles, and neurofibroma were present. The histopathologic examination of the biopsy sample taken from the dark brown macular lesions showed an increased number of melanocytes at the basal layer and were hence diagnosed as lentigo simplex. One of the close differentials of the lesions can be nevus spilus. Nevus spilus shows increased number of basal melanocytes similar to a lentigo simplex. Darker maculopapular lesions are often junctional or compound nevi. On histopathologic examination of the biopsy sample taken from the dark brown macular lesions, the diagnosis was lentigo simplex. Therefore, the patient was evaluated as segmental lentiginosis. The ophthalmologic examination showed multiple Lisch nodules smaller than 1 mm in diameter, present in the superior half of the iris in the ipsilateral eye [Figure 3]. No other pathologic finding was detected during neurological, orthopedic, and any other system examinations . Hemogram and biochemistry studies were within normal limits. There was no history of similar lesions in the other members of her family.
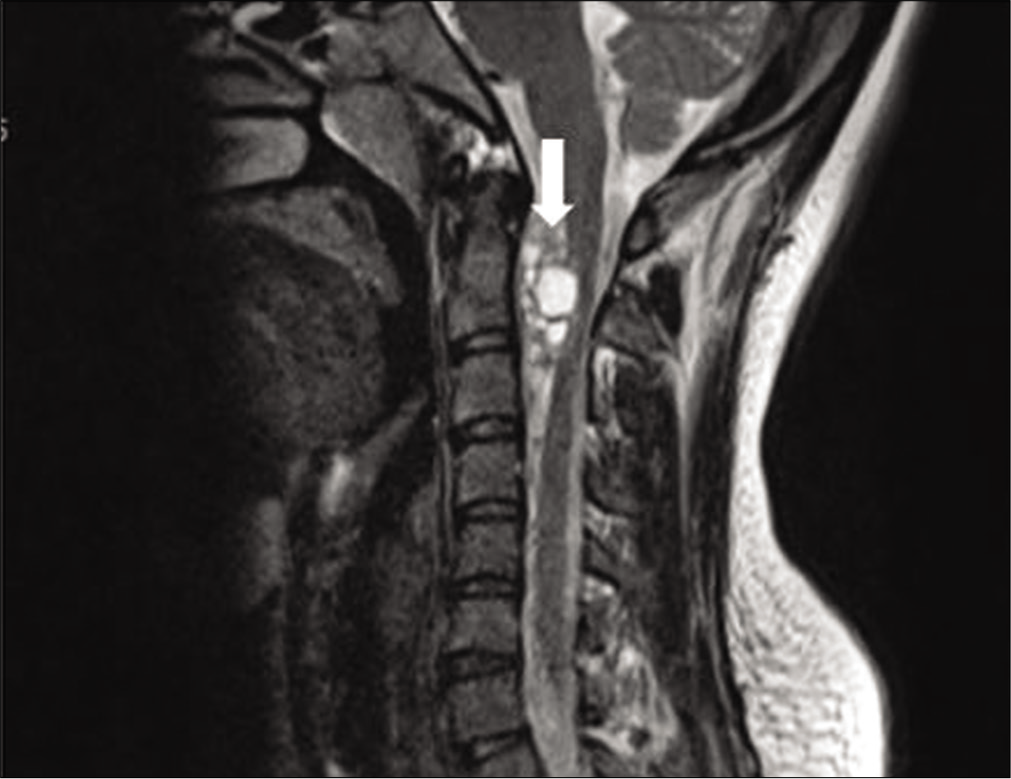
- A cystic mass with intradural localisation (white arrow), at the level of cervical 13 vertebra, 38 mm × 8 mm diameter (T2 based magnetic resonance imagingimages)

- A number of dark brown macular lesions of 2–3 mm size on a sharply circumscribed light brown background on the right side of the face

- A number of dark brown macular lesions with 2–3 mm size on the sharply circumscribed light brown surface on the right scapula
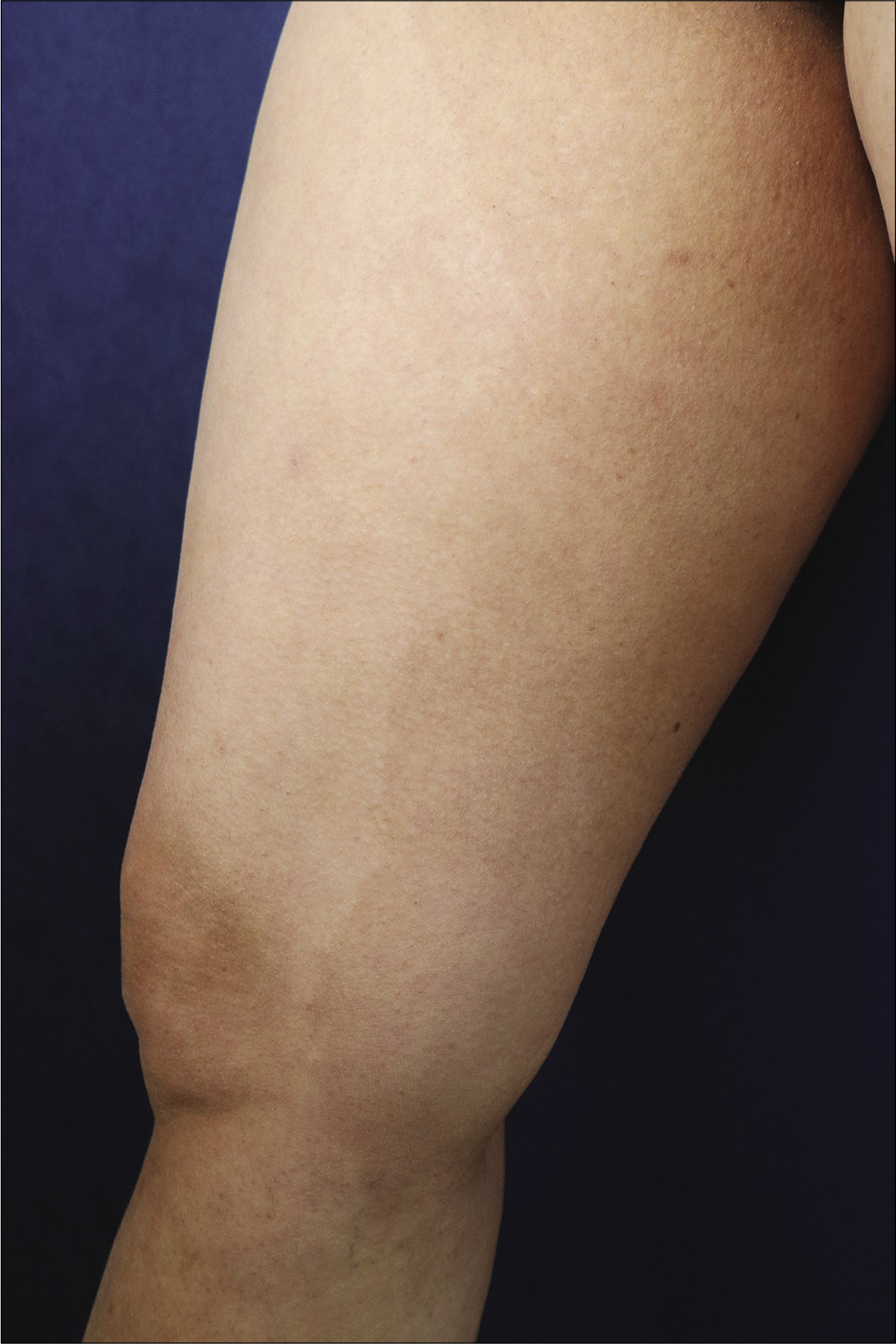
- A number of dark brown macular lesions with 2–3 mm size on the sharply circumscribed light brown surface on the medial aspect of right leg
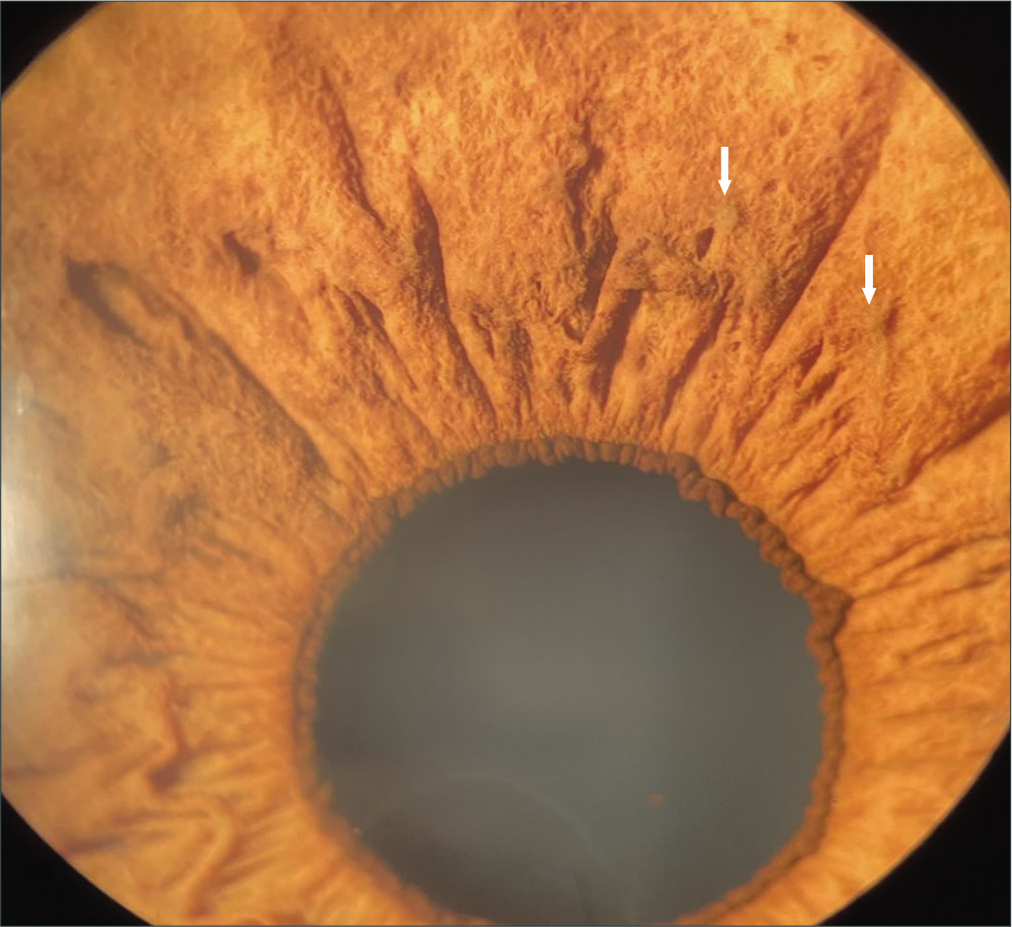
- A number of lisch nodules in the superior part of the iris (white arrows)
Unilateral segmental neurofibromatosis limited to a circumscribed body region, is a rare variant of neurofibromatosis. Mosaicism, which develops due to the post-zygotic mutation in the NF1 gene, has a role in its pathogenesis, and cutaneous findings of neurofibromatosis are detected in the affected circumscribed body region.3 The main clinical findings are cafe au-lait macules, axillary freckling and neurofibromas which affect one or several dermatomes limited to the midline.
Partial unilateral lentiginosis is characterized by numerous clustered lentigines on the normal skin. Histopathologically, they are sharply circumscribed lesions with lentigo characteristics, and clinically limited to the midline, involving one or several segments.
The association of partial unilateral lentiginosis and segmental neurofibromatosis is controversial. Some authors suggested that partial unilateral lentiginosis might be a form of segmental neurofibromatosis due to the accompanying findings such as axillary frecklings, cafe au-lait macules, and Lisch nodules in patients with partial unilateral lentiginosis.1,2 Ipsilateral Lisch nodules were detected accompanying lentiginosis lesions involving multiple segments on only one side of body in this patient. Similarly, similar cases accompanied by Lisch nodules have been reported in the literature. Chen et al. reported a case with accompanying cafe au-lait macules, axillary freckling, and lisch nodules in segmental lentiginosis.1
Neurofibromatosis is known to increase the tumor risk in patients, particularly in the central nervous system, and peripheral nerve sheath tumors. Pilocytic astrocytoma is a low-grade brain tumor originating from astrocytes. The association of pilocytic astrocytoma with NF1 has been reported, and the role of genetic mutation in tumorogenesis demonstrated.4 In addition, there exists evidence of the accompaniment of segmental neurofibromatosis, and malignancies, its association with neural crest originating tumors particularly malignant melanoma, and peripheral nerve sheath tumors in these patients.5 There is no reported data of the association of partial unilateral lentiginosis with malignancy except a melanoma case in literature.
Although there were no findings such as CALM, axillary freckling and neurofibroma in this patient, the presence of ipsilateral Lisch nodules and pilocytic astrocyoma pointing was suggestive of segmental neurofibromatosis. More published data and genetic studies that will reveal the mutation, are required to make a clear interpretation of this association. In addition, more detailed dermatologic, neurologic, and ophthalmologic examinations must be performed keeping in mind this possibility, and the patients must be followed-up for the possibility of later development of further systemic and ophthalmologic findings.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that name and initials will not be published and due efforts will be made to conceal the identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Partial unilateral lentiginosis with ipsilateral Lisch nodules and axillary freckling. Dermatology. 2004;209:321-4.
- [CrossRef] [PubMed] [Google Scholar]
- Agminated lentiginosis or segmental neurofibromatosis: A diagnostic challenge. Indian J Dermatol Venereol Leprol. 2016;82:75-7.
- [CrossRef] [PubMed] [Google Scholar]
- Genetic and clinical mosaicism in a patient with neurofibromatosis type 1. Hum Genet. 2004;114:284-90.
- [CrossRef] [PubMed] [Google Scholar]
- Neurofibromatosis type 1 associated low grade gliomas: A comparison with sporadic low grade gliomas. Crit Rev Oncol Hematol. 2016;104:30-41.
- [CrossRef] [PubMed] [Google Scholar]
- Segmental neurofibromatosis and cancer: Report of triple malignancy in a woman with mosaic Neurofibromatosis 1 and review of neoplasms in segmental neurofibromatosis. Dermatol Online J. 2016;22:8.
- [Google Scholar]




