Translate this page into:
Patch testing experience with 1000 patients
2 Department of Dermatology and STD, MLN Medical College, Allahabad, India
Correspondence Address:
A K Bajaj
Bajaj Skin Clinic, 3/6, Panna Lal Road, Allahabad, UP
India
| How to cite this article: Bajaj A K, Saraswat A, Mukhija G, Rastogi S, Yadav S. Patch testing experience with 1000 patients. Indian J Dermatol Venereol Leprol 2007;73:313-318 |
Abstract
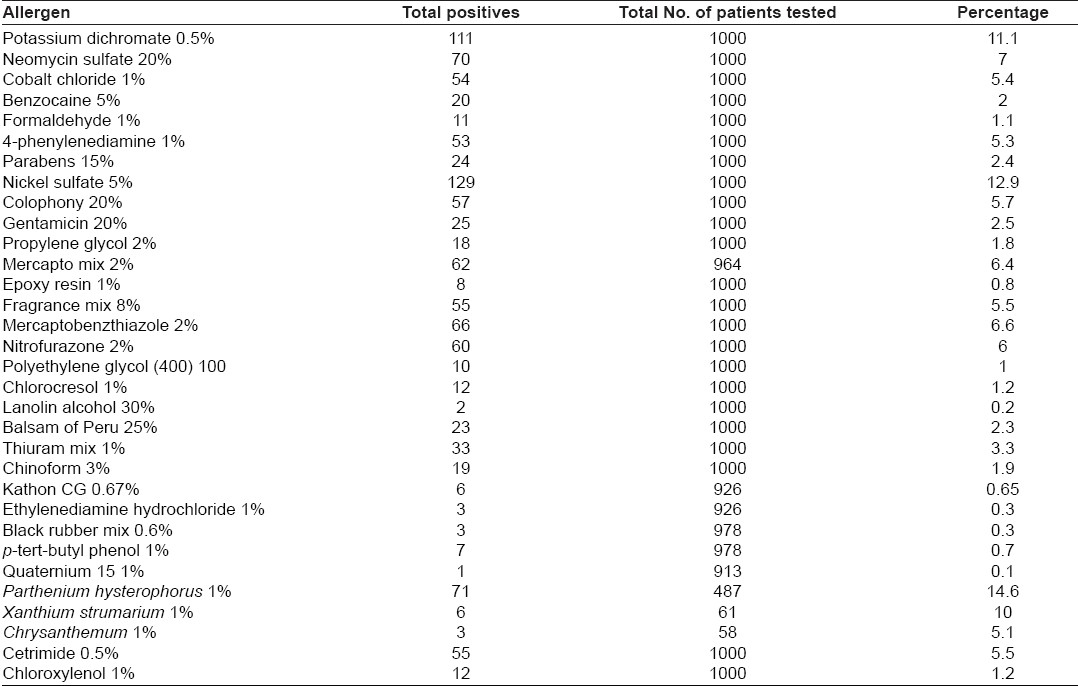
Background: Patch testing is a definitive tool for diagnosing allergic contact dermatitis (ACD). It reveals the prevalence and trends of contact sensitization in the community, thereby paving the way for better standard series. There is paucity of large series of patch-tested patients from India. Aim: To report the 9-year patch-test data from a single general dermatology centre in North India. Methods: Consecutive patients presenting with signs/symptoms of suspected ACD were patch tested from May 1997 to April 2006. The Indian Standard Series was used. Parthenium was tested only in selected patients and cetrimide and chloroxylenol were added to the series. Results: In total, records of 1000 patients (566 male, 434 female) were analyzed, yielding 1155 positive reactions in 590 (59%) patients. Footwear dermatitis was the commonest suspected diagnosis, followed by ACD to medicaments, cosmetic dermatitis and plant dermatitis. Out of the allergens that were tested in all the patients, positivity to nickel was the commonest (12.9%), followed by potassium dichromate (11.1%) neomycin (7%), mercaptobenzthiazole (6.6%), nitrofurazone (6%), colophony (5.7%), fragrance mix (5.5%) and cobalt chloride (5.4%). However, parthenium was the commonest allergen based on the proportion of patients tested with it (14.5%). In men, potassium dichromate (30%) was the commonest sensitizer and in women, nickel (43%) was the commonest to show patch-test positivity. Conclusion: Our study revealed higher prevalence of footwear and medicament dermatitis in comparison to existing data. Allergy to antiseptics is significant in our patients. Further collaborative studies involving patients from other parts of India are required to have an overall view of ACD in India.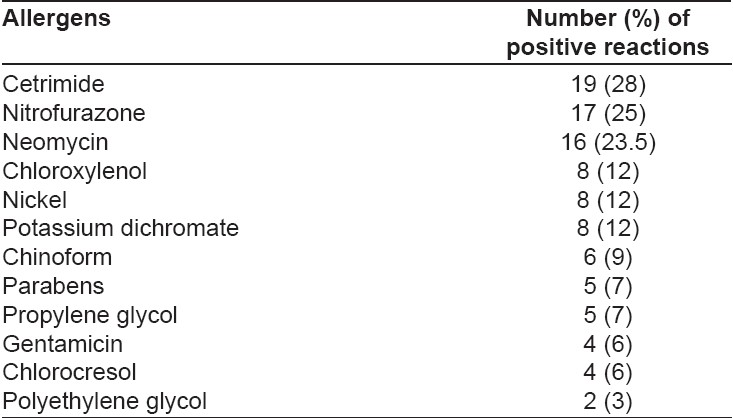
Introduction
As human life becomes increasingly complex, our skin is exposed to an ever-increasing spectrum of chemical and biological products. Inevitably, the incidence of allergic sensitization is showing a steady rise. A recent study of the general population from an area of Norway [1] reported sensitization rates as high as 35.4% in women and 14.8% in men. There have been no large-scale population-based studies of contact sensitization in our country; however, with rapid industrialization, westernization of society and poor labeling laws, India is ready for a contact sensitization "explosion."
Allergic contact dermatitis (ACD) develops in only a small proportion of sensitized individuals and population estimates vary from 1.7 [2] to 6%. [3] However, the true incidence of ACD in a society is very difficult to estimate since its diagnosis depends on several factors such as the demographic profile of patients, local industrial development, index of suspicion of the physician, and availability of patch testing. Common sensitizers also vary with place, patient profile and over the passage of time. Since optimal treatment of patients with ACD is predicated on accurate advice about prevention, regular patch testing followed by estimation of relevance is imperative in all suspected cases. We present herein our experience with patch testing in dermatology clinic attendees at a single centre at Allahabad in North India over a 9-year period.
Methods
A total of 1003 patients with suspected ACD were involved in this retrospective analysis of records. As a part of our standard protocol, demographic variables, clinical history, pattern of dermatitis and clinical diagnosis were recorded. The Indian Standard Series (ISS) was used for patch testing with the following modifications: Plant antigens were tested only in patients who were strongly suspected of having plant dermatitis based on history and clinical examination. Products brought by the patient himself were also used for testing whenever appropriate. Some initial patients were tested with a preliminary version of ISS that had fewer allergens. Cetrimide (0.5% aq.) and chloroxylenol (1% pet) were added to the patch-test battery based on the personal experience of the author (AKB) regarding local sensitivity patterns.
Patches were applied to the upper back using aluminium patch-test chambers mounted on a micropore tape. They were removed after 2 days and readings were taken on day 2 and day 4 for majority of the patients. Grading of the reactions was performed based on the ICDRG guidelines and only those reactions that persisted till day 3 or day 4 were considered to be positive. Relevance (present, past, probable or unknown) was established by a post-patch test interview of the patients. It was ascertained whether the dermatitis was chronologically and clinically congruent with the following: exposure (present relevance), past exposure (past relevance), exposure at any time probable (probable relevance), or indeterminate exposure (unknown relevance).
Results
Over a period of 9 years from May 1997 to April 2006, 1003 patients were included in the study; three of them were excluded from the final analysis due to the positive reactions to the control test chamber. The age of the remaining 1000 patients ranged from 8 years to 87 years with a median of 35.9 years. There were 566 males and 434 females. A total of 590 (59%) patients (336 males, 254 females) showed positivity to one or more allergens. Of these, 13 reacted only to their own product(s). There were no statistically significant differences between the sensitization rates in males and that in females. Nickel was the commonest allergen in women, with 109 of the 254 (43%) women showing positive reactions of being sensitive to it. In men, potassium dichromate was the predominant allergen with 100 of 338 (30%) reacting to it.
Suspected footwear dermatitis was the commonest clinical pattern in 310 patients, followed by suspected medicament dermatitis in 101 patients, cosmetic dermatitis in 88 patients, plant (airborne) dermatitis in 86 patients, atopic dermatitis in 76 patients, hand dermatitis in 71 patients, infective eczema in 39 patients. Other unclassified patterns of dermatitis were observed in 229 patients.
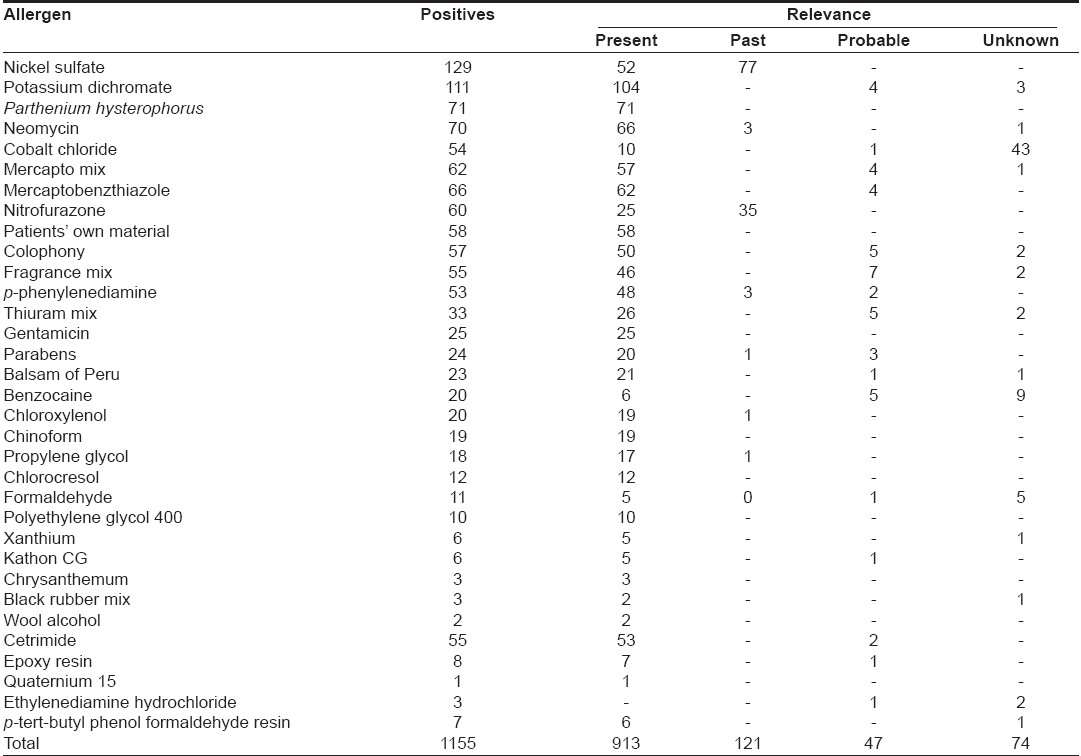
Positive reactions were noted to all the allergens tested [Table - 1]. The maximum numbers of positive reactions (49.6%) were recorded in the age range of 21 to 40 years. The most frequent sensitizers were parthenium (14.6%), nickel sulfate (12.9%), potassium dichromate (11.1%), neomycin (7.0%), mercaptobenzthiazole (6.6%) and nitrofurazone (6.0%). Out of the 1155 positive reactions, relevance to the present episode of dermatitis was established in 913 (79%) patients. Relevance data is mentioned in detail in [Table - 2]. Out of the 71 parthenium-positive patients, 63 (88.7%) had the classical airborne pattern of dermatitis. Rest of the parthenium-positive patients had disseminated photosensitive dermatitis (2 patients), generalized dermatitis (2 patients), atopic dermatitis (2 patients) and hand dermatitis (2 patients).
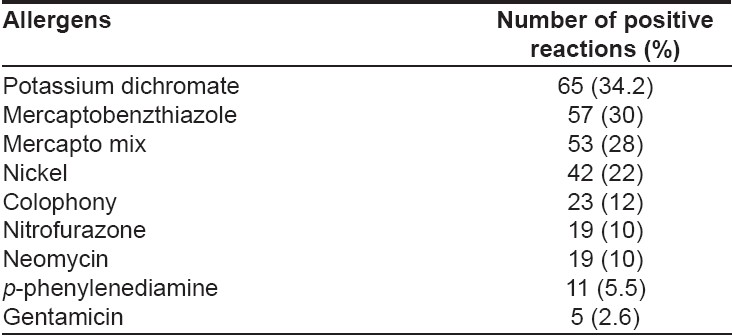
Among the 310 patients with suspected footwear dermatitis, 190 (61.3%) showed positivity to one or more allergens. Details of positivity in these patients are presented in [Table - 3]. A higher rate of patch-test positivity (68%) was observed in patients with dermatitis medicamentosa, who showed positivity to 12 different allergens [Table - 4].
In metal allergic patients, 52 (41.4%) of patients showing positivity to nickel had relevance to the current dermatitis, whereas 59.6% had past relevance correlating with ear piercing. On the other hand, 93.6% of chromate sensitive reactions had obvious relevance to the present dermatitis. Out of the 111 chromate-sensitive patients, 66 (59.5%) had footwear dermatitis, 22 (19.8%) had construction-work related hand/foot dermatitis and the rest had other patterns of dermatitis. Cobalt positivity was associated in all cases with concurrent positivity to nickel (41.8%), potassium dichromate (71%) or both nickel and potassium dichromate (23.6%).
Discussion
Almost 60% of all patch-tested patients in this study had one or more positive reactions. This figure is much higher than the positivity rate of 32.3% that was reported recently from Turkey in a very similar study [4] conducted over a comparable period. However, prior studies from other parts of India [5],[6] have reported patch-test positivity rates comparable to those seen in our patients. Our tropical climate may be partly responsible for this phenomenon. A more prosaic reason is possibly the low overall rate of patch testing in our patients, owing to the inconvenience and loss of wages associated with the three visits in 4 days that are required for this procedure. This would lead to artificially high rates of patch-test positivity, since only the more clinically suggestive patients would be submitted to patch testing. This also explains the relatively higher relevance rate (79%) observed in this study in comparison to the reports from western countries. Interestingly, recent reports from India have reported even higher relevance rates. [6]
There was no statistically significant difference in the sensitization rates between males and females in this study group. In contrast, many prior studies , have reported higher rates of patch-test positivity in females [7],[8] and some in males. [9] Most of this disparity between the sexes can be accounted for by the high rates of nickel positivity in women due to ear piercing. This trend was also observed in our patients with almost 85% (109 out of 129) of nickel-positive patients being women. However, in this study, 100 out of the 111 (90%) chromate-sensitive patients were men and this nullified the effect of the sex disparity in nickel sensitivity.
Similar to this study, high rates of chromate positivity have also been reported by Sharma et al. [7] from Chandigarh. Western countries have reported a sharp decline in chromate positivity since the addition of ferrous sulfate to cement, which converts the easily absorbable hexavalent chromium to the less-sensitizing trivalent form. [10] In France, the removal of chromium from a popular brand of household bleach resulted in a dramatic decline in chromate sensitivity in women. [11] However, in our patients, the main source of chromium was from leather footwear. Wearing thick absorbent socks and using other nonchromate chemicals for tanning and curing leather can minimize this form of exposure.
In this study, the commonest clinical pattern was footwear dermatitis followed by medicament and airborne contact dermatitis. In contrast, most of the large studies from abroad report hand dermatitis as the commonest pattern. [12],[13],[14] This difference may be due to variations in local culture, customs, occupational factors and climate. For instance, footwear dermatitis may be common in our patients due to poor quality of tanning of the leather, the practice of wearing shoes without socks and a hot and humid climate. Chemicals such as potassium dichromate (34.2%), mercaptobenzthiazole (30%) and mercapto mix (28%) were the leading allergens in patients with footwear dermatitis in our cohort. A significant number of these patients also reacted to topical antimicrobials. The emergence of topical medicaments, particularly antibiotics as important allergens in patients with foot dermatitis has also been documented recently by Holden and Gawkrodger [15] from England and Rani et al. [16] from Pakistan.
Prior Indian studies from North India have reported airborne (parthenium) dermatitis as the leading pattern, [6],[7] while some have found hands and/or feet [5] dermatitis to be the most frequent sites affected. In our series, parthenium dermatitis is under-represented in numerical terms in spite of being the commonest pattern seen in the clinic. This is because less than half of the patients with parthenium dermatitis were tested with it. Even then, it was proportionately the commonest allergen in our series. Because many parthenium sensitive patients presented with a highly distinct pattern of dermatitis, testing was not performed due to the risk of very strongly positive reactions. Sometimes the dermatitis was so unremitting that corticosteroids could not be sufficiently lowered to patch test them. Men predominated in the parthenium sensitive group with 61% of the parthenium-positive patients being males. This male predominance has been reported earlier by several workers. [5],[6],[7] and reflects greater outdoor exposure in men. Similar to our findings, Sharma et al. recently reported the varied clinical patterns of parthenium dermatitis viz. classical airborne, chronic actinic dermatitis type and mixed type. [17] They postulated that the differing patterns of parthenium dermatitis are a function of time; dermatitis always starts as the classical airborne pattern and gradually changes to an actinic or mixed pattern. While this is probably true in many cases, in our opinion, clinical pattern of parthenium dermatitis possibly depends on other factors such as occupation, clothing pattern, underlying atopy and route of (re)exposure. It has been argued by Mahajan et al. [18] that a generalized pattern of dermatitis in these patients may be the result of systemic, possibly inhalational exposure resulting in a systemic contact dermatitis.
Other compositae plants such as xanthium and chrysanthemum were tested in relatively few patients (~5%) in our cohort based on the history of specific exposure.
In this study, medicament dermatitis was the second most common diagnosis, which has been a relatively a small subset in prior studies of general dermatology patients. [5],[6],[7] Our patch-test yield was increased by the inclusion of cetrimide and chloroxylenol in the series, which accounted for an additional 67 positive reactions. Out of these, 27 patients had clearly relevant medicament exposure leading to the present dermatitis. We added cetrimide to our series based on our earlier study in which it was found to be a significant source of dermatitis medicamentosa. [19] In most of the cases in this study, exposure was related to Savlon, which contains cetrimide and chlorhexidine gluconate. Cetrimide positivity was observed in 55 (5.5%) patients; this is much higher than the most reported series involving a recent multicentric study from France. [20] However, a recent study of 50 patients with cosmetic dermatitis from Rohtak, India [21] reported cetrimide positivity in 12.2% cases. These high rates of cetrimide allergy may reflect increasingly indiscriminate use of antiseptic agents in bath water and as a final rinse while washing clothes. However, cetrimide can produce irritant reactions at the concentration used by us (0.5%) [22] and inclusion of some mild irritant reactions in our cases cannot be ruled out.
Chloroxylenol is the active ingredient of the popular antiseptic Dettol ® and it also cross-reacts with the preservative chlorocresol. [23] In our series, 12 (1.2%) patients each reacted to chloroxylenol and chlorocresol with four patients reacting to both the allergens.
Among antimicrobials, neomycin and nitrofurazone were the leading allergens, with 7% and 6% positivity respectively, followed by gentamicin (2.5%). However, nitrofurazone use has declined over the years but its widespread use in the past [19] in adhesive bandages and ointments still contributes to significant patch-test positivity. Reflecting this trend, nitrofurazone positivity in our patients was due to past topical exposure to the drug in almost 60% of positive patients. The rising use of topical gentamicin and neomycin was also reflected by high rates of positivity to these antimicrobials. In contrast to nitrofurazone, positive reactions to neomycin and gentamicin were relevant to the present exposure in more than 90% of cases.
Patients with hand eczema had a less than 50% positivity rate in our study with majority of them showing positivity to nickel. Nickel is a well-known cause of hand eczema and both topical and systemic exposure have been linked to it. [24]
To conclude, patch testing at our centre over the past 9 years has revealed that the commonest allergens in our patient population are parthenium, nickel, potassium dichromate and neomycin. Significant positivity is still observed with nitrofurazone despite its decreasing use and the rise in gentamicin positivity. Antiseptics such as cetrimide and chloroxylenol are also important allergens in our patient population. These agents merit further testing in other areas of the country and if significant positivity rates are found, a case for their inclusion in the ISS can be made. In view of the differences in clinical patterns, positivity rates etc. reported from different parts of India, we owe it to our patients to clarify the epidemiology of this important problem. A multicentric study from all the major geographic areas of the country is required to initiate further studies in this matter.
| 1. |
Dotterud LK, Smith-Sivertsen T. Allergic contact sensitization in the general adult population: A population-based study from Northern Norway. Contact Dermatitis 2007;56:10-5.
[Google Scholar]
|
| 2. |
Rietschel RL, Fowler Jr. JF. In: Fisher's Contact Dermatitis. 4 th ed. Philadelphia: Lippincott Williams & Wilkins: 1995.
th ed. Philadelphia: Lippincott Williams & Wilkins: 1995.'>[Google Scholar]
|
| 3. |
Johnson ML, Johnson KG, Engel A. Prevalence, morbidity and cost of dermatological diseases. J Am Acad Dermatol 1984;11:930-6.
[Google Scholar]
|
| 4. |
Akyol A, Boyvat A, Peksari Y, Gurgey E. Contact sensitivity to standard series allergens in 1038 patients with contact dermatitis in Turkey. Contact Dermatitis 2005;52:333-7.
[Google Scholar]
|
| 5. |
Singhal V, Reddy BS. Common contact sensitizers in Delhi. J Dermatol 2000;27:440-5.
[Google Scholar]
|
| 6. |
Sharma VK, Sethuraman G, Garg T, Verma KK, Ramam M. Patch testing with the Indian standard series in New Delhi. Contact Dermatitis 2004;51:319-21.
[Google Scholar]
|
| 7. |
Sharma VK, Chakrabarti A. Common contact sensitizers in Chandigarh, India. A study of 200 patients with the European standard series. Contact Dermatitis 1998;38:127-31.
[Google Scholar]
|
| 8. |
Hammershoy O. Standard patch test results in 3225 consecutive Danish patients from 1973 to 1977. Contact Dermatitis 1980;6:263-8.
[Google Scholar]
|
| 9. |
Akhtar N, Rashid MM, Chowdhury AQ, Ali E, Chowdhury AM. Patch test for the detection of contact allergens. Mymensingh Med J 2004;13:181-4.
[Google Scholar]
|
| 10. |
Zachariae CO, Agner T, Menne T. Chromium allergy in consecutive patients in a country where ferrous sulphate has been added to cement since 1981. Contact Dermatitis 1996;35:83-5.
[Google Scholar]
|
| 11. |
Lachapelle JM, Lauwerys R, Tennstedt D, Anadanson J, Benezra C, Chabaeu G, et al . Eau de Javel and prevention of chromate allergy in France. Contact Dermatitis 1980;6:107-10.
[Google Scholar]
|
| 12. |
al-Sheikh OA, Gad el-Rab MO. Allergic contact dermatitis: Clinical features and profile of sensitizing allergens in Riyadh, Saudi Arabia. Int J Dermatol 1996;35:493-7.
[Google Scholar]
|
| 13. |
Holness DL, Nethercott JR, Adams RM, Belsito D, Deleo V, Emmett EA, et al . Concomitant positive patch test results with standard screening tray in North America, 1985-1989. Contact Dermatitis 1995;32:289-92.
[Google Scholar]
|
| 14. |
Lestringant GG, Bener A, Sawaya M, Galadari IH, Frossard PM. Allergic contact dermatitis in the United Arab Emirates. Int J Dermatol 1999;38:181-6.
[Google Scholar]
|
| 15. |
Holden CR, Gawkrodger DJ. Ten years' experience of patch testing with a shoe series in 230 patients: Which allergens are important? Contact Dermatitis 2005;53:37-9.
[Google Scholar]
|
| 16. |
Rani Z, Hussain I, Haroon TS. Common allergens in shoe dermatitis: Our experience in Lahore, Pakistan. Int J Dermatol 2003;42:605-7.
[Google Scholar]
|
| 17. |
Sharma VK, Sethuraman G, Bhat R. Evolution of clinical pattern of parthenium dermatitis: A study of 74 cases. Contact Dermatitis 2005;53:84-8.
[Google Scholar]
|
| 18. |
Mahajan VK, Sharma NL, Sharma RC. Parthenium dermatitis: Is it a systemic contact dermatitis or an airborne contact dermatitis? Contact Dermatitis 2004;51:231-4.
[Google Scholar]
|
| 19. |
Bajaj AK, Gupta SC. Contact hypersensitivity to topical antibacterial agents. Int J Dermatol 1986;25:103-5.
[Google Scholar]
|
| 20. |
Barbaud A, Vigan M, Delrous JL, Assier H, Avenel-Audran M, Collet E, et al . Contact allergy to antiseptics: 75 cases analyzed by the dermato-allergovigilance network. Ann Dermatol Venereol 2005;132:962-5.
[Google Scholar]
|
| 21. |
Tomar J, Jain VK, Aggarwal K, Dayal S, Gupta S. Contact allergies to cosmetics: Testing with 52 cosmetic ingredients and personal products. J Dermatol 2005;32:951-5.
[Google Scholar]
|
| 22. |
Lee JY, Wang BJ. Contact dermatitis caused by cetrimide in antiseptics. Contact Dermatitis 1995;33:168-71.
[Google Scholar]
|
| 23. |
Burry JN, Kirk J, Reid J, Turner T. Chlorocresol sensitivity. Contact Dermatitis 1975;1:41-2.
[Google Scholar]
|
| 24. |
Christensen OB, Moller H. Nickel allergy and hand eczema. Contact Dermatitis 1975;1:129-35.
[Google Scholar]
|
Fulltext Views
3,923
PDF downloads
2,693





![[Table - 1]](#tbl_ijdvl_2007_73_5_313_34008_1.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2007_73_5_313_34008_2.jpg){kind=link}
![[Table - 3]](#tbl_ijdvl_2007_73_5_313_34008_3.jpg){kind=link}
![[Table - 4]](#tbl_ijdvl_2007_73_5_313_34008_4.jpg){kind=link}