Translate this page into:
Penicillamine-induced elastosis perforans serpiginosa with abnormal "lumpy-bumpy" elastic fibers in lesional and non-lesional skin
Correspondence Address:
Rachita S Dhurat
B 14/2, Maitri Park Co. Op. Hsg. Soc. Sion Trombay Road, Chembur, Mumbai - 400 071
India
| How to cite this article: Khatu SS, Dhurat RS, Nayak CS, Pereira RR, Kagne RB. Penicillamine-induced elastosis perforans serpiginosa with abnormal "lumpy-bumpy" elastic fibers in lesional and non-lesional skin. Indian J Dermatol Venereol Leprol 2011;77:55-58 |
Abstract
Four types of elastosis perforans serpiginosa (EPS) have been described in literature: 1) idiopathic EPS, 2) reactive perforating elastosis associated with connective tissue disorders, 3) in some instances of pseudoxanthoma elasticum (PXE), disease-specific calcified elastic tissue is extruded, producing a clinical picture indistinguishable from other types, may also be seen in patients undergoing hemodialysis and 4) EPS induced by long-term treatment with D-penicillamine is observed in patients suffering from Wilson's disease. Long term D-penicillamine therapy causes an alteration in the dermal elastic tissue. D-penicillamine induced EPS has a distinctive histopathologic feature - serrated appearance of elastic fibers due to perpendicular budding from their surface giving a "lumpy-bumpy" look. D-penicillamine induced elastic fiber alteration may not always manifest clinically as EPS. We report a case of D-penicillamine induced widespread alteration in skin elastic tissue with distinct histopathologic features.Introduction
D-penicillamine is a heavy metal chelator primarily used for disorders such as Wilson′s disease, cystinuria and juvenile rheumatoid arthritis. D-penicillamine induced degenerative dermatoses include cutis laxa, anetoderma, pseudoxanthoma elasticum (PXE), elastosis perforans serpiginosa (EPS), ecchymoses, and lymphangiectasis. [1] Penicillamine-induced EPS shows distinct histopathologic changes of "lumpy-bumpy" elastic fibers in the dermis of lesional and non-lesional skin, as compared to idiopathic EPS. [2]
Case Report
A 26-year-old man presented in April 2009 with 1-year history of asymptomatic raised skin lesions initially on the nape of the neck and then on both sides of the neck [Figure - 1] and inner aspect of thighs and left forearm, with a gradual increase in size and central clearing. He was a diagnosed case of Wilson′s disease and was under treatment with oral penicillamine 500 mg twice daily since the last 18 years (1991). The patient was otherwise well. On cutaneous examination, there were multiple skin-colored to brownish colored papules coalescing to form serpiginous plaques varying in size from 1 to 10 cm with central clearing, atrophy and hypopigmentation and raised hyperkeratotic rim. Individual papules had a crateriform appearance with elevated edge and central keratinous plug.
 |
| Figure 1 :Brown papules coalescing to form serpiginous plaques with central clearing, atrophy and raised hyperkeratotic rim over sides of the neck |
All his vital parameters were stable. Central nervous system examination revealed dysarthria and dystonia. No Kayser-Fleischer rings were seen on ophthalmologic examination. Serum and urinary copper levels were raised on multiple occasions. Liver biopsy in 2003 was suggestive of macronodular cirrhosis. Magnetic resonance imaging of the brain showed atrophy of the caudate nucleus and putamen in the year 2003. Lesional skin biopsy from the raised border demonstrated markedly acanthotic epidermis with a transepidermal wavy channel containing thick, coarse elastic fibers and granular basophilic material along with mononuclear inflammatory infiltrate. Abundant, abnormal, clumped, elastic fibers were present in the middle and upper dermis in the vicinity of the channel [Figure - 2]. These were confirmed to be elastic fibers on staining with Verheoff-van Gieson stain [Figure - 3]. At higher magnification (400Χ), the striking feature of presence of multiple serrations and buds arising perpendicularly from the borders of the elastic fibers [Figure - 4] was seen. Similar lumpy-bumpy elastic fibers were observed in perilesional and distant clinically normal looking skin, although the budding and serration were less prominent.
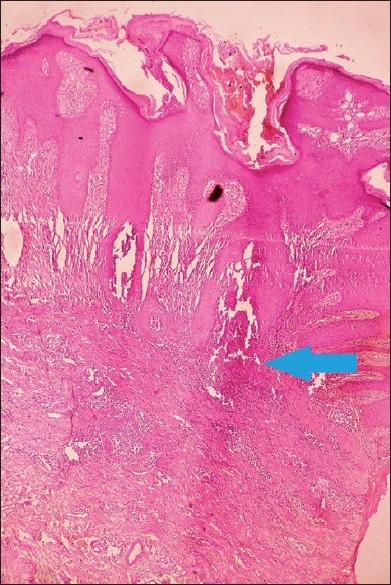 |
| Figure 2 :Lesional skin showing markedly acanthotic epidermis with a transepidermal wavy channel (H and E, ×40) |
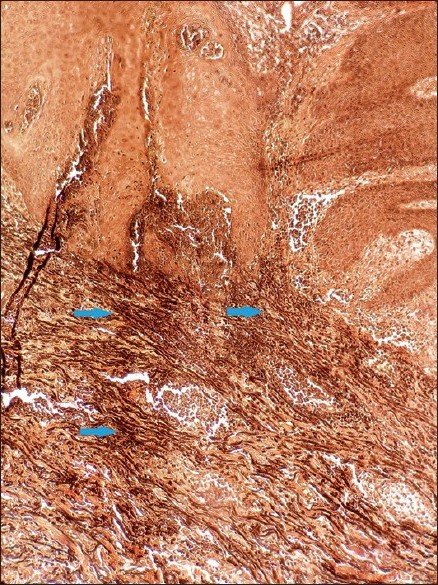 |
| Figure 3 :Abnormal elastic fibers (Verheoff-van Gieson stain, ×40) |
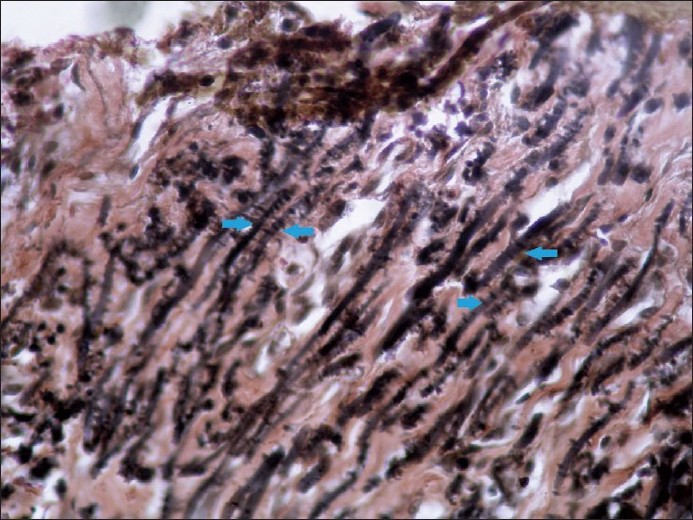 |
| Figure 4 :"Lumpy-bumpy" elastic fibers with perpendicular serrations from their surface (lesional skin, Verheoff-van Gieson stain, ×400) |
Thus, the diagnosis of penicillamine-induced EPS was made. There was no improvement in lesions after 2 months of topical tazarotene. The patient was treated with 40 mg/ml of triamcinolone acetonide intralesionally which resulted in improvement in the lesions after three such injections.
Discussion
EPS, also called perforating elastoma or elastoma intrapapillare perforans, is a reactive perforating dermatosis in which elastic fibers are extruded through the epidermis. It is a rare disorder that affects young individuals, with a peak incidence in the second decade of life. Men are affected more often than females. The exact cause is unknown, but a genetically determined defect of elastic tissue is hypothesized. Primary abnormality is possibly in the dermal elastin, which provokes a cellular response that leads to extrusion of abnormal elastic tissue. [3] Since its first delineation as a separate entity (Lutz 1953, Miescher 1955), EPS has been shown to cover four different types of connective tissue disease: 1) idiopathic or primary EPS, 2) reactive perforating elastosis associated with connective tissue disorders such as PXE, Ehlers-Danlos syndrome, Marfan′s syndrome, osteogenesis imperfecta and Down′s syndrome, 3) in some instances of PXE, disease-specific calcified elastic tissue is extruded, producing a clinical picture indistinguishable from other types, and may also seen in patients undergoing hemodialysis and 4) a distinctive type is that induced by long-term treatment with penicillamine is observed in patients suffering from Wilson′s disease. [4]
Long-term d-penicillamine therapy causes multiple degenerative changes in elastic fibers of skin. Similar elastic fiber changes have been reported in upper respiratory tract, [5] pulmonary tissue, [4] aortic wall, visceral adventitia and alveolar septa. [4] Abnormal elastic fibers are not only confined to lesional skin, but also present in non-lesional skin. [4]
The mechanism by which penicillamine disrupts elastin production or remodeling is uncertain. One proposed mechanism involves the copper-dependent enzyme, lysyl oxidase, that is required for the cross linkage of elastic fibers in the dermis. Penicillamine, by chelating the copper cofactor, indirectly inhibits lysyl oxidase activity, allowing abnormal elastic fiber accumulation. These thickened elastic fibers act as mechanical irritants or "foreign bodies" and provoke the epidermal response in the form of epidermal hyperplasia. The epidermis then envelops the irritating material and eliminates it through transepidermal channels. [6],[7],[8] These changes are dose-dependent and do not seem to occur with doses under 2 g/day. The severe dermal elastosis may be present without cutaneous signs of EPS. [4]
Idiopathic as well as d-penicillamine induced EPS clinically manifest as small, horny, umbilicated papules arranged in lines, circles or segments of circles in a serpiginous pattern. The individual papule has characteristic craterifom appearance with an elevated edge and central keratinous plug. Lesions may persist for several years but eventually involute spontaneously to leave atrophic scars. Back and sides of the neck, face, and flexor surface of upper extremities are more commonly involved. [3] An unusual occurrence of penicillamine-induced mucosal lesions has been reported. [9]
In EPS induced by penicillamine, characteristic changes are seen in lesional and non-lesional skin. Elastic fibers, mainly of the reticular dermis, are coarser, serrated with saw-tooth like borders and with perpendicular budding from the surface. Non-penicillamine induced EPS shows elastic fibers that are clumped, curly, frayed, fragmented, thickened and granular. [4] In addition, histologic features common to other forms of EPS include a narrow transepidermal channel that may be straight, wavy or corkscrew shaped. Thick, coarse elastic fibers are seen in the channel admixed with granular basophilic debris and mixed inflammatory infiltrate. Epidermis surrounding the fully developed lesion is acanthotic and hyperkeratotic. In the dermis beneath and around the lesion, there are abnormal elastic fibers and foreign body giant cell reaction. [7] Similarly, in our case, the elastic fibers in middle and deep dermis were grossly altered with numerous serrations on their surface. Electron microscopy shows an increase in the number of elastic fibers.
Numerous treatment modalities have been described, although none is considered as the gold standard. Moderately effective treatments include cryotherapy, oral isotretinoin, and cellophane tape stripping. Topical tazarotene gel and imiquimod cream have demonstrated fair improvement in lesions. Tazarotene may aid in unplugging transepidermal canals of EPS. Imiquimod may modulate immune response to an elastin antigen. [9] Excision and dermabrasion should be avoided. Response to treatment varies widely and discontinuation of penicillamine therapy does not guarantee absence of the dermatosis in the future.
| 1. |
Faghihi G, Ali A, Wali A. Cutaneous side-effects of D-penicillamine. Indian J Dermatol 2003;48:133-6.
[Google Scholar]
|
| 2. |
Gebhart W, Bardach H. The "lumpy-bumpy" elastic fiber. A marker of long-term administration of penicillamine. Am J Dermatopathol 1981;3:33-9.
[Google Scholar]
|
| 3. |
Burrows NP, Lovell CR. Disorders of connective tissue. In: Burns T, Breathnach S, Cox N, Griffiths C, editors. Rook's Textbook of Dermatology. 7 th ed. Oxford: Blackwell Publishing; 2004. p. 46.66-7.
th ed. Oxford: Blackwell Publishing; 2004. p. 46.66-7.'>[Google Scholar]
|
| 4. |
Bardach H, Gebhart W, Niebauer G. "Lumpy-bumpy" elastic fibers in the skin and lungs of a patient with a penicillamine-induced elastosis perforans serpiginosa. J Cutan Pathol 1979;6:243-52.
[Google Scholar]
|
| 5. |
Manohar MB, Boldy DA, Bryan RL, Pearman K. Penicillamine-induced changes in elastic tissue of the upper respiratory tract. J Laryngol Otol 1993;107:62-4.
[Google Scholar]
|
| 6. |
Seymour CA. Trace metal disorders. In: Weatherall DJ, Ledingham JG, Warrell DA, editors. Oxford Textbook of Medicine. 3 rd ed. Oxford: Oxford University Press; 1996. p. 1417-9.
[Google Scholar]
|
| 7. |
Narayan N, Nousari C, Heilman E, Freidman R. Degenerative diseases and perforating disorders. In: Elder D, Elenitsas R, Johnson B, Murphy G, editors. Lever's histopathology of the skin. 10 th ed. Philadelphia: Lippincott Williams and Wilkins; 2005. p. 393-5.
th ed. Philadelphia: Lippincott Williams and Wilkins; 2005. p. 393-5.'>[Google Scholar]
|
| 8. |
Rath N, Bhardwaj A, Kar HK, Sharma PK, Bharadwaj M, Bharija SC. Penicillamine-induced pseudoxanthoma elasticum with elastosis perforans serpiginosa: A case report. Indian J Dermatol Venereol Leprol 2005;71:182-5.
[Google Scholar]
|
| 9. |
Lewis B, Chern P, Stone M. Penicillamine-induced elastosis of the mucosal lip. J Am Acad Dermatol 2009;60:700-3.
[Google Scholar]
|
Fulltext Views
4,019
PDF downloads
2,746





![[Figure - 1]](#fig_ijdvl_2011_77_1_55_74982_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2011_77_1_55_74982_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2011_77_1_55_74982_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2011_77_1_55_74982_f4.jpg){kind=link}