Translate this page into:
Phototherapy for atopic dermatitis
Correspondence Address:
Sunil Dogra
Department of Dermatology, Venereology and Leprology, Postgraduate Institute of Medical Education and Research, Chandigarh - 160 012
India
| How to cite this article: Dogra S, Mahajan R. Phototherapy for atopic dermatitis. Indian J Dermatol Venereol Leprol 2015;81:10-15 |
Abstract
Background: The aim of these guidelines is to review the available published literature regarding the effectiveness of phototherapy and photochemotherapy in atopic dermatitis and put forward recommendations regarding their use in atopic dermatitis. Materials and Methods: A literature search was performed to collect data from PubMed, EMBASE, and the Cochrane Library published till March 2014. Keywords used were "phototherapy", "photochemotherapy", "NB-UVB", "BBUVB", "PUVA", "UVA1", "atopic dermatitis", and "atopic eczema". Systematic reviews, meta-analysis, national guidelines, randomized controlled trials, prospective open label studies, and retrospective case series in English literature mentioning use of above-mentioned keywords were reviewed. Results: Six hundred and eighty eight studies were evaluated, 38 of which fulfilled the criteria for inclusion in the guidelines. Conclusions and Recommendations: Both UV1 and narrow-band UVB are effective in significantly decreasing the eczema severity although UV1 may be preferred in acute flares and narrow-band UVB in chronic eczema, especially in adults (Level of evidence 1+, Grade of recommendation A). Among various doses of UVA1, medium dose UVA1 may be preferred over others as its efficacy is similar to high dose and better than low dose UVA1 phototherapy. Narrow-band UVB is preferred to broad-band UVB (Level of evidence 1+, Grade of recommendation A). Medium-dose UVA1 is similar in efficacy to narrow-band UVB (Level of evidence 1+, Grade of recommendation A). In children, despite its efficacy, narrow-band UVB phototherapy should be used only as a second line therapy due to its potential for long-term adverse effects (Level of evidence 2+, Grade of recommendation B).INTRODUCTION
Atopic dermatitis (AD) is an inflammatory, chronically remitting and relapsing pruiritic dermatosis with a prevalence of 2-5%. [1] ′Atopy′ has been defined as ′a personal or familial tendency to produce IgE antibodies in response to low doses of allergens, usually proteins, and to develop typical symptoms such as asthma, rhinoconjunctivitis or eczema/dermatitis′. [2] Management can be challenging and involves short-term control of acute symptoms with topical corticosteroids/topical calcineurin inhibitors, and oral corticosteroids in severe disease, reducing disease flares and avoidance of drug-related side effects. Various types of photo (chemo) therapy that have been tried include psoralen plus ultraviolet A(UVA) (PUVA) therapy, UVA1 phototherapy (high-dose [HD], medium-dose [MD], and low-dose [LD]), UVA/B phototherapy, narrow-band (NB-UVB) phototherapy and broad-band UVB (BBUVB) phototherapy.
Phototherapy is considered a second-line treatment in the management of atopic dermatitis, especially in adults; that is, it can be tried in patients in whom the disease is not adequately controlled with emollients and topical corticosteroids/immunomodulators. [3],[4],[5],[6] The European Task Force on atopic dermatitis (ETFAD) does not recommend the use of phototherapy for children under 12 years because of the potential long-term side effects. [4] Pure UVA therapy has a limited role although the newer UVA-1 devices that emit moderate-to-high doses in a shorter time have shown efficacy in patients with acute and recalcitrant atopic dermatitis. [7],[8] The action of UVA-1 is mediated through T lymphocyte apoptosis and decreased expression of interferon g (IFN-γ) by activated T cells. Photochemotherapy, which involves combination of UVA with psoralens (PUVA), can be administered orally (hence called systemic PUVA) or topically (bath- or cream-PUVA).
Goals of the guidelines
The aim of the guidelines is to review the available published literature regarding the effectiveness of phototherapy and photochemotherapy in atopic dermatitis and on this basis, put forth guidelines for their use in this disease.
Materials and Methods
A literature search was performed to collect data on the use of phototherapy in the treatment of atopic dermatitis. Relevant literature published till March 2014 was obtained from PubMed, EMBASE, and the Cochrane Library. Keywords like "phototherapy", "photochemotherapy", "NBUVB", "BBUVB", "PUVA", "UVA1", "atopic dermatitis", and "atopic eczema" were used for literature search. All systematic reviews, meta-analysis, national guidelines, randomized controlled trials (RCT), prospective open label studies, and retrospective case series in English literature were reviewed.
Evaluation of the literature
The levels of evidence and grades of recommendations for each guideline were according to the format
suggested by the British Association of Dermatologists. [9] The studies selected were assessed for their methodology as per the NICE Technical Manual and graded using a code ′++′, ′+′ or ′-′, based on the extent to which potential biases were minimized. Thereafter, the grade of recommendation was made.
RESULTS
A total of 428 studies were evaluated, 38 of which fulfilled the criteria for inclusion in the guidelines.
BBUVB phototherapy
In the initial study by Jekler and Larko involving, 17 patients with half-side comparison between BBUVB (0.5-1.0 minimal erythema dose [MED]) and visible light, the former was found to be significantly better. The second part of study by the same authors compared the therapeutic dose response to UVB (0.8 MED versus 0.4 MED applied to one-half of the body). Both UVB doses were found to be effective with no significant differences. [10] Hannuksela et al. utilized Psorilux 9050 emitting UVB and UVA at an ouput of 1.24 mW/cm 2 at 280-315 nm and 7.33 mW/cm 2 at 315-400 nm to treat 107 atopic patients and found both the treatment modalities to be beneficial in 93% of cases with a significant corticosteroid-sparing effect (Level of evidence 2+). [11] In another paired comparison study of 21 patients (Level of evidence 2+), UVA was shown to be significantly better than BBUVB for the total clinical score (P < 0.02), the overall evaluation score (P < 0.01) and the extent of dermatitis (P < 0.05). [12]
NB-UVB phototherapy
Several studies have clearly demonstrated the effectiveness of NB-UVB for in atopic dermatitis. In a study of 21 adults with severe disease, air-conditioned NB-UVB photo-therapy three times weekly for 12 weeks led to a 68% reduction in disease severity and an 88% reduction in topical corticosteroid use, and 15 out of 21 patients continued to show benefit 24 weeks after discontinuing NB-UVB. [13] In a randomised controlled trial, 73 patients were randomized to receive either NB-UVB, broadband UVA or visible light phototherapy twice weekly for 12 weeks. NB-UVB was demonstrated to be very effective in moderate-to-severe adult atopic dermatitis with remission lasting for 3 months (Level of evidence 1+). In comparison, broadband UVA phototherapy was only moderately beneficial. [14] However, this study did not demonstrate a significant corticosteroid-sparing effect of either irradiation regimens as has been reported in earlier studies. [13] In another half-side comparative trial between NB-UVB and PUVA by der-Petrossian
et al., both led to a similar decrease in mean baseline SCORAD (scoring atopic dermatitis) index. [15] No acute severe adverse effects were reported. Treatment with oral short-term cyclosporin A for 4 weeks, followed by a washout phase of 4-6 weeks and subsequent NB-UVB phototherapy (3 times/week, up to 2 months) has been reported to be effective in the treatment of severe atopic dermatitis. [16] Legat et al. compared NB-UVB with medium dose UVA1 using half-side comparison in nine patients with chronic atopic dermatitis and observed 40% reduction of Costa score with NB-UVB and a better reduction of pruritus compared to medium dose UVA1. [17] However, more recent trials demonstrated NB-UVB and medium dose UVA1 to be equally effective in the treatment of moderate-to-severe AD (Level of evidence 1++). [18],[19]
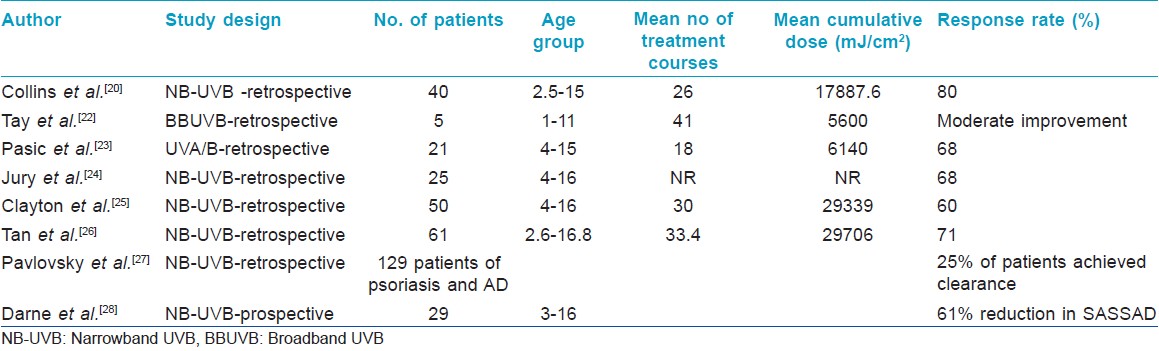
The effect of NB-UVB has been also evaluated in children and has been found to be an effective and well-tolerated treatment modality. [Table - 1]. [20],[21],[22],[23],[24],[25],[26],[27] In a retrospective study of 25 children with atopic dermatitis, Jury et al. reported that 68% of children achieved near complete clearance after treatment. [24] However, the study did not comment on the eczema severity, length of remission, or whether topical treatment was continued during treatment with NB-UVB. In the first prospective study assessing the efficacy of NB-UVB phototherapy in 29 children aged 3-16 years, 61% reduction in mean SASSAD (Six Area Six Sign Atopic Dermatitis) score was seen in the NB-UVB cohort compared with an increase of disease severity in the unexposed cohort with significant reduction in subjective and quality of life scores (P < 0.05). [26] In another 6-year retrospective study of 50 children, NB-UVB phototherapy (along with topical corticosteroids) led to clearance or minimal residual activity in 40% of patients in 3 months. [25]
UVA/B Phototherapy
Combination phototherapy of UVA and UVB irradiation can be applied by using special tubes whose emission spectrum includes both ranges or by combining UVA and UVB tubes simultaneously or in a serial manner. Valkova and Velkova demonstrated that combination UVA/B and topical corticosteroids was significantly better than UVA/B alone for the reduction of treatment duration (P = 0.02). [28] Granlund et al.[29] showed that ciclosporin was significantly better than UVA/B for the rapid reduction of SCORAD (P < 0.001 in week 2, 4, and 6 of cycle 1), the days in remission (P < 0.01) and the improvement in quality of life during the first 4 weeks of treatment (P < 0.01). In the two paired comparison studies by Jekler and Larko, combined UVA/B phototherapy was observed to be better than monotherapy with either low dose UVB or UVA phototherapy. [30],[31]
Photochemotherapy
In a recent study by Tzaneva et al., 5-methoxypsoralen (MOP) PUVA was found to be significantly better than medium dose UVA1 in reducing the disease severity (P = 0.04) and increasing the duration of remission (P = 0.01; Level of evidence 1-). [32] In another small, half-side comparison study, no significant difference was seen between bath PUVA (using 8-MOP) and NB-UVB for a decrease of SCORAD either directly after treatment or after a follow-up period up to 1 year (week 2, P = 0.09; week 4, P = 0.51; week 6, P = 0.48; 1 year, P value not mentioned). [15] In a large randomised controlled trial, Heinlin et al. observed that synchronous balneo phototherapy with NB-UVB was significantly better than NB-UVB alone for the reduction of SCORAD at the end of the treatment period (P < 0.004) and at 6 months (P < 0.04; Level of evidence 1++). [33]
UVA-1 phototherapy
In a pilot study of UVA-1 irradiation, Krutman et al. compared UVA-1 phototherapy (given in a single dose of 130J /cm 2 for 15 consecutive days) with UVA/B irradiation (starting doses 30 mJ/cm 2 UVB and 7 J/cm 2 UVA, respectively). [34] The authors found UVA-1 to be significantly more effective compared with UVA/B therapy in reducing the clinical scores and in the downregulation of eosinophilic cationic protein levels. Later, a multicenter follow-up study with more patients established the superiority of high dose UVA-1 high-dose therapy over topical corticosteroids and UVA/B therapy. [35] Similarly, medium dose UVA-1 cold light (50 J/cm 2 /day for 15 days) led to a significant reduction of the SCORAD score and cytokine receptor levels in atopic eczema. [36],[37],[38]
In a half-side comparison of high dose versus medium dose UVA-1 irradiation by Tzaneva et al., high dose UVA-1 irradiation (130 J/cm 2 /day for 15 days) led to a 35% and medium dose UVA-1 (65 J/cm 2 /day for 15 days) to a 28% decrease in the SCORAD score. [39] In an earlier randomised controlled trial by Dittmar et al., comparing low-dose (20 J/cm 2 ), medium dose (65 J/cm 2 ), and high dose (130 J/cm 2 ) UVA-1, [40] it was found that the medium dose and high dose treatment regimens were superior to the low-dose UVA-1 regimen. However, there were no significant differences between the high dose and the medium dose cohorts and the tolerability was higher in the medium dose group (Level of evidence 1+). Medium dose UVA-1 is as effective as high dose UVA-1 for the treatment of patients with severe atopic dermatitis. In another study, medium dose UVA-1 cold light (45 J/cm2, 5 times weekly for 4 weeks) showed prolonged therapeutic improvement in disease activity and quality of life. [41] In another study, 15 irradiation cycles of medium dose UVA-1 phototherapy induced healing of the lesions in chronic vesicular dyshidrotic hand eczema. in 10 out of 12 patients with no relapse till 3 months. [42]
NB-UVB and medium dose UVA1 are equally effective in the treatment of patients with moderate-to-severe atopic dermatitis. [15] In a randomized investigator-blinded trial, Majoie et al. evaluated 13 adults (aged 20-56 years) with chronic atopic dermatitis and found NB-UVB and medium dose UVA1 to be equally effective in reducing disease severity. [14] Similar results have been seen by other authors. [14],[15],[43],[44] In a comparative crossover study of phototherapy modalities, 28 patients completed separate 6-week courses of both UVA1 and NB-UVB phototherapy. Both therapies were equally effective in significantly decreasing scores for pruritus and clinical severity (Level of evidence 1+). [19] In a multicenter study of 53 patients, high dose UVA1 was significantly more effective than treatment with either fluocortolone or combined UVA-UVB therapy (Level of evidence 1+). [35] However, there has been no direct comparison of efficacy of UVA1 in ′acute′ versus ′chronic′ eczema.
Most studies have reported no serious adverse effects with UVA1 phototherapy. [6] Most notably, the frequency of UV-induced burning seems to be lower for UVA1 than for conventional UVB or PUVA. Adverse effects reported included xerosis, erythema, and burning of the skin. Less commonly reported side-effects were pruritus (UVA1 and full-spectrum light), gastrointestinal diseases (balneophototherapy), exacerbations of eczema (UVA, NB-UVB, visible light, full-spectrum light), folliculitis (UVA1, PUVA), and photo-onycholysis (PUVA).
DISCUSSON
Based on the review of available literature, it may be deduced that among the various modalities administered as phototherapy, medium dose UVA1 and NB-UVB phototherapy are the most effective as observed in various randomized controlled trials and half-body paired comparon studies. While the former may be used for controlling acute flares of atopic dermatitis, NB-UVB is the most effective in managing chronic disease. Moreover, since high dose UVA1 and medium dose UVA1 has been shown to have similar efficacy, the latter may be the preferred option as the amount to heat produced is less leading to better patient acceptability. Due to paucity of evidence, full-spectrum UVA, BB-UVB and full-spectrum light should not be recommended for the treatment of atopic dermatitis. However, more data needs to be generated before phototherapy is prescribed more routinely for this indication. It may also be noted that among the various studies reviewed, there was considerable clinical and methodological heterogeneity with differences in the quality of studies. Moreover, many studies reported the concomitant use of topical corticosteroids, which further confounds the results. Another important aspect is the limited availability of UV1 phototherapy and moreover, considering its high cost, its usefulness in a developing country like India is questionable. Phototherapy may not be beneficial for all patients as some may not tolerate the associated heat and sweating and hence, the treatment needs to be individualized.
Adverse effects of phototherapy also need to be evaluated in greater detail. Although most studies do not report any significant side effects, UVA1 phototherapy has been associated with hyperpigmentation, redness, dryness, pruritus, herpes simplex virus reactivation and the induction of polymorphic light eruption. Studies of chronic UVA1 effects in humans are limited but may include photoaging and possible photocarcinogenesis. In atopic dermatitis, long-term safety data of PUVA have not been investigated so far. Reports of skin cancer in patients treated with UVA1 are usually confounded with the use of other therapies known to also increase the risk of cutaneous malignancies. For instance, a case of melanoma was reported in a patient with mastocytosis after receiving UVA1 treatment, however, this individual had also received PUVA bath therapy in the past. [45] In addition, there are two cases of Merkel cell carcinoma after UVA1 phototherapy but both patients had blood dyscrasias and were treated with immunosuppressants. [46] New devices, such as 308 nm monochromatic excimer light expand the therapeutic options in patients with localized and therapy-resistant disease, even though they can treat only limited areas. [47],[48],[49]
| 1. |
Wüthrich B. Clinical aspects, epidemiology, and prognosis of atopic dermatitis. Ann Allergy Asthma Immunol 1999;83:464-70.
[Google Scholar]
|
| 2. |
Johansson SG, Cardell LO, Foucard T, Montan P, Odebäck P, Palmqvist M, et al. Revised, global nomenclature for allergy. Unambiguous terms create clarity and prevent misunderstandings. Lakartidningen 2006;103:379-83.
[Google Scholar]
|
| 3. |
Darsow U, Wollenberg A, Simon D, Taïeb A, Werfel T, Oranje A. ETFAD/EADV eczema task force 2009 position paper on diagnosis and treatment of atopic dermatitis. J Eur Acad Dermatol Venereol 2010;24:317-28.
[Google Scholar]
|
| 4. |
Ring J, Alomar A, Bieber T, Deleuran M, Fink-Wagner A, Gelmetti C, et al. Guidelines for treatment of atopic eczema (atopic dermatitis) Part II. J Eur Acad Dermatol Venereol 2012;26:1176-93.
[Google Scholar]
|
| 5. |
Silverberg JI. Atopic Dermatitis: An Evidence-Based Treatment Update. Am J Clin Dermatol 2014;15:149-64.
[Google Scholar]
|
| 6. |
Garritsen FM, Brouwer MW, Limpens J, Spuls PI. Photo (chemo) therapy in the management of atopic dermatitis: An updated systematic review with implications for practice and research. Br J Dermatol 2014;170:501-13.
[Google Scholar]
|
| 7. |
Grundmann SA, BeissertS. Modern aspects of phototherapy for atopic dermatitis. J Allergy (Cairo) 2012;2012:121797.
[Google Scholar]
|
| 8. |
Zandi S, Kalia S, Lui H. UVA1 Phototherapy: A Concise and Practical Review. Skin Therapy Lett 2012;17:1-4.
[Google Scholar]
|
| 9. |
Bell HK, Ormerod AD; BAD Therapy and Guidelines Subcommittee. Writing a British Association of Dermatologists clinical guideline: An update on the process and guidancefor authors. Br J Dermatol 2009;160:725-8.
[Google Scholar]
|
| 10. |
Jekler J, Larkö O. UVB phototherapy of atopic dermatitis. Br J Dermatol 1988;119:697-705.
[Google Scholar]
|
| 11. |
Hannuksela M, Karvonen J, Husa M, Jokela R, Katajamäki L, Leppisaari M. Ultraviolet light therapy in atopic dermatitis. Acta Dermato-Venereologica 1985;65:137-9.
[Google Scholar]
|
| 12. |
Jekler J, Larkö O. UVA solarium versus UVB phototherapy of atopic dermatitis: A paired-comparison study. Br J Dermatol 1991;125:569-72.
[Google Scholar]
|
| 13. |
George SA, Bilsland DJ, Johnson BE, Ferguson J. Narrow-band (TL-01) UVB air-conditioned phototherapy for chronic severe adult atopic dermatitis. Br J Dermatol 1993;128:49-56.
[Google Scholar]
|
| 14. |
Reynolds NJ, Franklin V, Gray JC, Diffey BL, Farr PM. Narrow-band ultraviolet B and broad-band ultraviolet A phototherapy in adult atopic eczema: A randomised controlled trial. Lancet 2001;357:2012-6.
[Google Scholar]
|
| 15. |
Der-Petrossian M, Seeber A, Hönigsmann H, Tanew A. Half-side comparison study on the efficacy of 8-methoxypsoralen bath-PUVA versus narrow-band ultraviolet B phototherapy in patients with severe chronic atopic dermatitis. Br J Dermatol 2000;142:39-43.
[Google Scholar]
|
| 16. |
Brazzelli V, Prestinari F, Chiesa MG, Borroni RG, Ardigò M, Borroni G. Sequential treatment of severe atopic dermatitis with cyclosporin a and low-dose narrow-band UVB phototherapy. Dermatology 2002;204:252-4.
[Google Scholar]
|
| 17. |
Legat FJ, Hofer A, Brabek E. Narrowband UV-B vs medium-dose UV-A1 phototherapy in chronic atopic dermatitis. Arch Dermatol 2003;139:223-4.
[Google Scholar]
|
| 18. |
Majoie IM, Oldhoff JM, van Weelden H, Laaper-Ertmann M, Bousema MT, Sigurdsson V, et al. Narrowband ultraviolet B and medium-dose ultraviolet A1 are equally effective in the treatment of moderate to severe atopic dermatitis. J Am Acad Dermatol 2009;60:77-84.
[Google Scholar]
|
| 19. |
Gambichler T, Othlinghaus N, Tomi NS, Holland-Letz T, Boms S, Skrygan M, et al. Medium-dose ultraviolet (UV) A1 vs narrowband UVB phototherapy in atopic eczema: A randomized crossover study. Br J Dermatol 2009;160:652-8.
[Google Scholar]
|
| 20. |
Collins P, Ferguson J. Narrowband (TL-01) UVB air-conditioned phototherapy for atopic eczema in children. Br J Dermatol 1995;133:653-5.
[Google Scholar]
|
| 21. |
Tay YK, Morelli JG, Weston WL. Experience with UVB phototherapy in children. Pediatr Dermatol 1996;13:406-9.
[Google Scholar]
|
| 22. |
Pasiæ A, Ceoviæ R, Lipozenciæ J, Husar K, Susiæ SM, Skerlev M, et al . Phototherapy in pediatric patients. Pediatr Dermatol 2003;20:71-7.
[Google Scholar]
|
| 23. |
Jury CS, McHenry P, Burden AD, Lever R, Bilsland D. Narrowband ultraviolet B (UVB) phototherapy in children. Clin Exp Dermatol 2006;31:196-9.
[Google Scholar]
|
| 24. |
Clayton TH, Clark SM, Turner D, Goulden V. The treatment of severe AD in childhood with narrowband ultraviolet B phototherapy. Clin Exp Dermatol 2007;32:28-33.
[Google Scholar]
|
| 25. |
Darné S, Leech SN, Taylor AE. Narrowband ultraviolet B phototherapy in children with moderate-to-severe eczema: A comparative cohort study. Br J Dermatol 2014;170: 150-6.
[Google Scholar]
|
| 26. |
Tan E, Lim D, Rademaker M. Narrowband UVB phototherapy in children: A New Zealand experience. Australas J Dermatol 2010;51:268-73.
[Google Scholar]
|
| 27. |
Pavlovsky M, Baum S, Shpiro D, Pavlovsky L, Pavlotsky F. Narrow band UVB: Is it effective and safe for paediatric psoriasis and atopic dermatitis? J Eur Acad Dermatol Venereol 2011;25:727-9.
[Google Scholar]
|
| 28. |
Valkova S, Velkova A. UVA/UVB phototherapy for atopic dermatitis revisited. J Dermatolog Treat 2004;15:239-44.
[Google Scholar]
|
| 29. |
Granlund H, Erkko P, Remitz A, Langeland T, Helsing P, Nuutinen M, et al. Comparison of cyclosporin and UVAB phototherapy for intermittent one-year treatment of atopic dermatitis. Acta Derm Venereol 2001;81:22-7.
[Google Scholar]
|
| 30. |
Jekler J, Larkö O. Phototherapy for atopic dermatitis with ultraviolet A (UVA), low-dose UVB and combined UVA and UVB: Two paired-comparison studies. Photodermatol Photoimmunol Photomed 1991;8:151-6.
[Google Scholar]
|
| 31. |
Jekler J, Larkö O. Combined UVA-UVB versus UVB phototherapy for atopic dermatitis: A paired-comparison study. J Am Acad Dermatol 1990;22:49-53.
[Google Scholar]
|
| 32. |
Heinlin J, Schiffner-Rohe J, Schiffner R, Einsele-Krämer B, Landthaler M, Klein A, et al. A first prospective randomized controlled trial on the efficacy and safety of synchronous balneophototherapy vs. narrow-band UVB monotherapy for atopic dermatitis. J Eur Acad Dermatol Venereol 2011;25:765-73.
[Google Scholar]
|
| 33. |
Tzaneva S, Kittler H, Holzer G, Reljic D, Weber M, Hönigsmann H, et al. 5-Methoxypsoralen plus ultraviolet (UV) A is superior to medium-dose UVA1 in the treatment of severe atopic dermatitis: A randomized crossover trial. Br J Dermatol 2010;162:655-60.
[Google Scholar]
|
| 34. |
Krutmann J, Czech W, Diepgen T, Niedner R, Kapp A, Schöpf E, et al. High-dose UVA1 therapy in the treatment of patients with atopic dermatitis. J Am Acad Dermatol 1992;26:225-30.
[Google Scholar]
|
| 35. |
Krutmann J, Diepgen TL, Luger TA, Grabbe S, Meffert H, Sönnichsen N, et al. High-dose UVA1 therapy for atopic dermatitis: Results of a multicenter trial. J Am Acad Dermatol 1998;38:589-93.
[Google Scholar]
|
| 36. |
Kowalzick L, Kleinheinz A, Weichenthal M, Neuber K, Köhler I, Grosch J, et al. Low dose versus medium dose UV-A1 treatment in severe atopic eczema. Acta Derm Venereol 1995;75:43-5.
[Google Scholar]
|
| 37. |
Von Kobyletzki G, Pieck C, Hoffmann K, Freitag M, Altmeyer P. Medium-dose UVA1 cold-light phototherapy in the treatment of severe atopic dermatitis. J Am Acad Dermatol 1999;41:931-7.
[Google Scholar]
|
| 38. |
Abeck D, Schmidt T, Fesq H, Strom K, Mempel M, Brockow K, et al. Long-term efficacy of medium-dose UVA1 phototherapy in atopic dermatitis. J Am Acad Dermatol 2000;42:254-7.
[Google Scholar]
|
| 39. |
Tzaneva S, Seeber A, Schwaiger M, Hönigsmann H, Tanew A. High-dose versus medium-dose UVA1 phototherapy for patients with severe generalized atopic dermatitis. J Am Acad Dermatol 2001;45:503-7.
[Google Scholar]
|
| 40. |
Dittmar HC, Pflieger D, Schöpf E, Simon JC. UVA1 phototherapy. Pilot study of dose finding in acute exacerbated atopic dermatitis. Hautarzt 2001;52:423-7.
[Google Scholar]
|
| 41. |
Polderman MC, Wintzen M, le Cessie S, Pavel S. UVA-1 cold light therapy in the treatment of atopic dermatitis: 61 patients treated in the Leiden University Medical Center. Photodermatol Photoimmunol Photomed 2005;21:93-6.
[Google Scholar]
|
| 42. |
Schmidt T, Abeck D, Boeck K, Mempel M, Ring J. UVA1 irradiation is effective in treatment of chronic vesicular dyshidrotic hand eczema. Acta Derm Venereol 1998;78:318-9.
[Google Scholar]
|
| 43. |
Grundmann-Kollmann M, Behrens S, Podda M, Peter RU, Kaufmann R, Kerscher M. Phototherapy for atopic eczema with narrow-band UVB. J Am Acad Dermatol 1999;40:995-7.
[Google Scholar]
|
| 44. |
Kerr AC, FergusonJ, Attili SK, Beattie PE, Coleman AJ, Dawe RS, et al. Ultraviolet A1 phototherapy: A British Photodermatology Group workshop report. Clin Exp Dermatol 2012;37:219-26.
[Google Scholar]
|
| 45. |
Trautinger F. Phototherapy of mycosis fungoides. Photodermatol Photoimmunol Photomed 2011;27:68-74.
[Google Scholar]
|
| 46. |
Gokdemir G, Barutcuoglu B, Sakiz D, Koslu A. Narrowband UVB phototherapy for early-stage mycosis fungoides: Evaluation of clinical and histopathological changes. J Eur Acad Dermatol Venereol 2006;20:804-9.
[Google Scholar]
|
| 47. |
Mavilia L, Mori M, Rossi R, Campolmi P, Puglisi Guerra A, Lotti T. 308 nm monochromatic excimer light in dermatology: Personal experience and review of the literature. G Ital Dermatol Venereol 2008;143:329-37.
[Google Scholar]
|
| 48. |
Wollenschläger I, Hermann J, Ockenfels HM. Targeted UVB-308 nm (NUVB) therapy with excimer laser in the treatment of atopicdermatitis and other inflammatory dermatoses. Hautarzt 2009;60:898-906.
[Google Scholar]
|
| 49. |
Mavilia L, Mori M, Rossi R. 308 nm monochromatic excimer light in dermatology: Personal experience and review of the literature. G Ital Dermatol Venereol 2008;143:329-37.
[Google Scholar]
|
Fulltext Views
8,632
PDF downloads
3,222





![[Table - 1]](#tbl_ijdvl_2015_81_1_10_148557_t1.jpg){kind=link}