
Translate this page into:
Pigmented Bowen’s disease on the finger mimicking malignant melanoma: A dermoscopic pitfall
-
Received: ,
Accepted: ,
How to cite this article: Cui Y, Wang ZY, Shen X. Pigmented Bowen’s disease on the finger mimicking malignant melanoma: A dermoscopic pitfall. Indian J Dermatol Venereol Leprol 2021;87:270-3.
Sir,
Pigmented Bowen’s disease, characterized by variable melanin deposition, constitutes 1.7%–5.5% of all Bowen’s disease.1 Involvement of finger is even rarer. We report a case of digital pigmented Bowen’s disease clinically and dermoscopically resembling melanoma. This is a special case depicting both atypical pigment network and peripheral parallel ridge pattern on dermoscopy, which may lead to the misdiagnosis of malignant melanoma.
A 49-year-old man (Fitzpatrick skin phototype IV) presented with a dark-brown lesion on the lateral aspect of his left ring finger, progressively enlarging for last 1 year. Slight lesional pain developed since three months. Physical examination revealed a well-demarcated, asymmetric, slightly elevated, dark brown plaque with scaly surface, sized 18 mm. [Figure 1]. The patient denied any prior treatment. There was no history of exposure to arsenic, tar, or radiation. Family and past history were unremarkable.
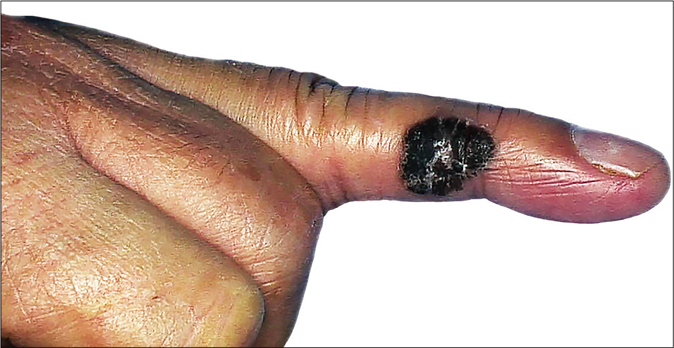
- Elevated, asymmetric dark brown plaque on the left ring finger with scaly surface, measuring 18 mm × 14 mm in size
Lesional dermoscopy demonstrated atypical pigment network with peripheral parallel ridge pattern over an asymmetric dark brown background. We also observed dotted vessels in clustered arrangement, regression-like areas, and linear ulceration. [Figure 2]. Melanocytic parameters such as atypical pigment network and parallel ridge pattern mandated a skin biopsy to rule out malignant melanoma. Histopathological examination revealed full-thickness epidermal dysplasia along with atypical keratinocytes [Figure 3a]. No dermal invasion was noted. However, we observed melanin granules within tumor cells and dermal melanophages [Figures 3b and c]. We diagnosed the case as pigmented Bowen’s disease after clinico-pathological correlation. We excised the plaque and no recurrence was detected at 11 months of follow-up.
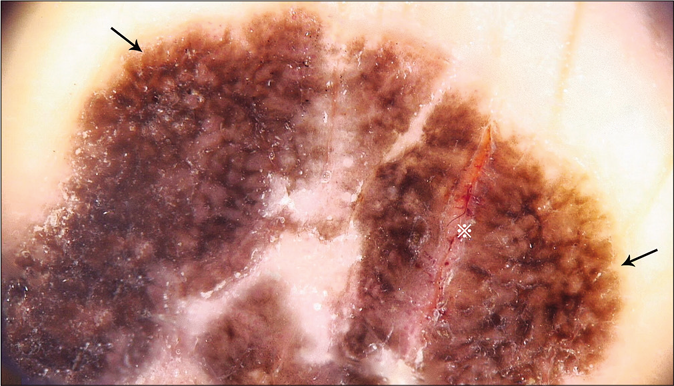
- Atypical pigment network (black arrows), linear ulceration (※)
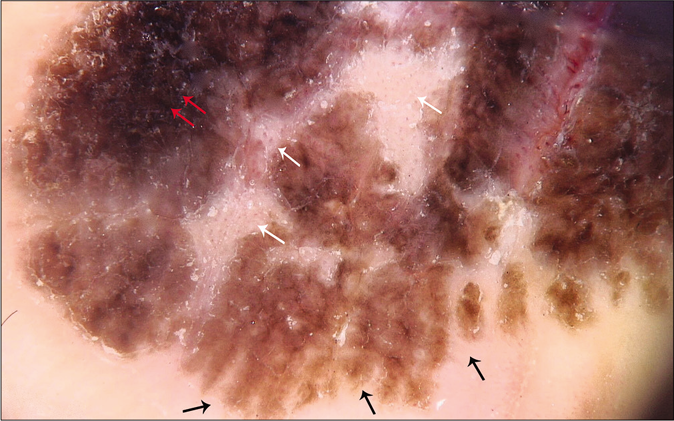
- Parallel ridge pattern (black arrows), dotted vessels on regression like areas (white arrows), and irregular blotch (red arrows). (non-polarized dermoscopy, ×20; Medicam 800, FotoFinder SystemsGmbh, Birbach, Germany)
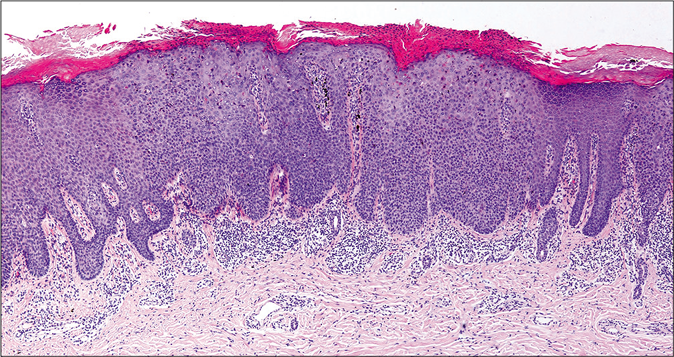
- Hyperkeratosis, parakeratosis, acanthosis and irregular elongation of rete ridges without atypical cells in the upper dermis were found (H and E, ×40)
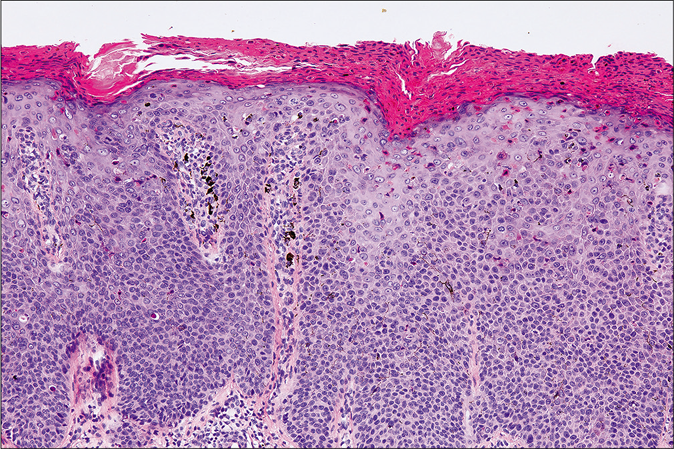
- Disorganized atypical keratinocytes throughout epidermis with densely distributed melanin granules (H and E, ×100)
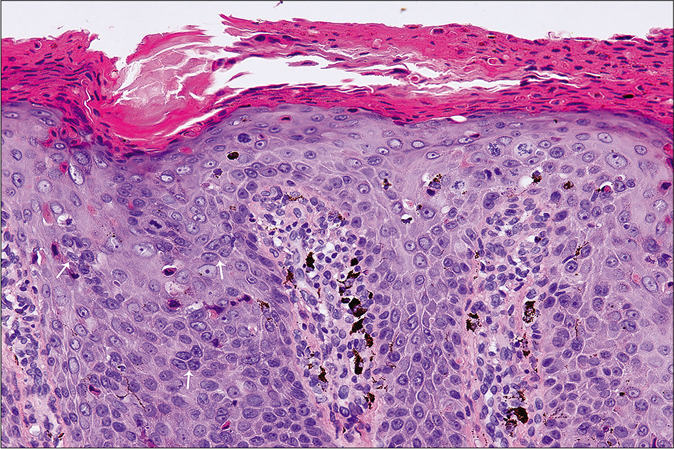
- Atypical mitotic figures (white arrows) and individual keratinized cells in the epidermis (H and E, ×400)
Previously reported characteristic dermoscopic patterns of 52 cases of pigmented Bowen’s disease included brown or grey dots and/or structureless brown zones, while “pigment network” was rare due to notable epidermal acanthosis along with loss of rete ridges.1 However, we noted atypical pigment network without the classical brown or grey dots. The lines of atypical pigment network and parallel ridge pattern occurred due to melanin deposits within tumoral cells and irregular thickening of rete ridges. The holes of pigment network represented dermal papillary tips. Our dermoscopic findings may also be attributed to the atypical site of lesion. Our findings corroborate the hypothesis that neoplastic cells probably induce the proliferation and activation of melanocytes, similar to melanocytic lesions.
Peripheral parallel ridge pattern is the dermoscopic hallmark of acral melanoma, while diffuse light brown pigmentation in early stages become focally darker in advanced lesions.2 BRAAFF checklist is a new dermoscopic algorithm to diagnose acral melanoma with 93.1% sensitivity and 86.7% specificity. The scoring system consists of six variables (blotches, ridge pattern, asymmetry of structures, asymmetry of colors, furrow pattern, and fibrillar pattern). We observed irregular blotches (1), ridge pattern (3), asymmetry of structures and colors (2) without furrow pattern and fibrillar pattern to obtain a BRAAFF score of 6, highly suggestive of acral melanoma [Table 1].3
| Dermoscopic features | Pigmented Bowen’s disease (our case) | Acral melanoma | Pigmented Bowen’s disease (common cases) |
|---|---|---|---|
| Irregular blotch | + | + | - |
| Parallel ridge pattern | + | + | - |
| Asymmetry of structures | + | + | - |
| Asymmetry of colors | + | + | - |
| Atypical network | + | + | - |
| Regression structures | + | + | - |
| Fibrillar pattern | - | - | - |
| Parallel furrow pattern | - | - | +/- |
| Brown/grey dots | - | +/- | + |
| Structureless brown zones | - | +/- | + |
| Surface scale | + | - | + |
| Dotted vessels | + | - | + |
+: present, -: absent
Instead of parallel ridge pattern, parallel furrow pattern was reported in a case of palmar pigmented Bowen’s disease.4 Nakayama and colleagues also reported parallel furrow pattern in periungual disease without parallel ridge pattern (highly specific for diagnosing acral melanoma).5 Besides, parallel brown to gray radial lines have been reported in digital pigmented Bowen’s disease.6 Furthermore, patchy, irregular reticular pigmentation was demonstrated in two cases, but both were less pigmented than our case.7,8 Interestingly, we detected both distinct atypical pigment network and peripheral parallel ridge pattern in our patient.
We considered pigmented seborrheic keratosis, pigmented palmoplantar wart and acral melanocytic nevus as our differentials. A considerable number of pigmented Bowen’s disease occur in association with seborrheic keratosis and may constitute a collision tumor.1 Seborrheic keratosis presents with a waxy, scaly surface with characteristic “pasted on” look. The diagnosis of pigmented seborrheic keratosis can be challenging when its characteristic features are masked by heavy melanin deposition. However, cerebriform pattern, fingerprint pattern, comedo-like openings and milia-like cysts on dermoscopy are valuable markers for pigmented seborrheic keratosis. Occasionally such cases may also show “false” pigment network.9 Pigmented palmoplantar wart clinically presents as a pigmented, rough, sharply-defined plaque with slightly keratotic surface caused by human papilloma virus infection. Underlying black dots representing thrombosed capillaries on paring are confirmatory. Dermoscopic examination usually reveals tiny dotted vessels on a brownish background, but parallel ridge pattern has been reported in plantar pigmented wart.10 Most acquired acral melanocytic nevi present as round or spindle-shaped, well-circumscribed evenly pigmented brownish-black macules. However, our case presented with both asymmetric structures and colors. More than 75% of acral nevi exhibit one of these three major dermoscopic patterns: the parallel furrow, lattice-like and fibrillar patterns, neither was observed in our case.11
To conclude, we were unable to find any previous reports of pigmented Bowen’s disease showing both distinct atypical pigment network and peripheral parallel ridge pattern, which are typical dermoscopic features of malignant melanocytic lesions. Although the dermoscopic evidence of surface scales and dotted vessels are indicative of the condition, we misdiagnosed it as melanoma, till histology confirmed our final diagnosis. Therefore, histopathological examination remains the gold standard for diagnosis, as demonstrated by our case. We also recommend the inclusion of pigmented Bowen’s disease as differential diagnosis of any pigmented lesion, along with malignant melanoma.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that his name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Research on medical collaborative scientific and technological innovation (NO. Z19110700770000).
Conflicts of interest
There are no conflicts of interest.
References
- Dermatoscopy of pigmented Bowen's disease. J Am Acad Dermatol. 2010;62:597-604.
- [CrossRef] [PubMed] [Google Scholar]
- Early detection of acral melanoma: A review of clinical, dermoscopic, histopathologic, and molecular characteristics. J Am Acad Dermatol. 2019;81:805-12.
- [CrossRef] [PubMed] [Google Scholar]
- The BRAAFF checklist: A new dermoscopic algorithm for diagnosing acral melanoma. Br J Dermatol. 2015;173:1041-9.
- [CrossRef] [PubMed] [Google Scholar]
- Pigmented Bowen disease of the palm: An atypical case diagnosed by dermoscopy. J Am Acad Dermatol. 2010;62:356-7.
- [CrossRef] [PubMed] [Google Scholar]
- Dermoscopy of periungual pigmented Bowen's disease: Its usefulness in differentiation from malignant melanoma. J Eur Acad Dermatol Venereol. 2016;30:552-4.
- [CrossRef] [PubMed] [Google Scholar]
- High risk human papillomavirus in a child with digital pigmented Bowen's disease: Case report and dermoscopic findings. Pediatr Dermatol. 2018;35:e265-7.
- [CrossRef] [PubMed] [Google Scholar]
- Pigmented Bowen's disease associated with high risk HPV simulating melanoma of the hand. An Bras Dermatol. 2017;92:686-8.
- [CrossRef] [PubMed] [Google Scholar]
- Identification of a human papillomavirus type 58 lineage in multiple Bowen's disease on the fingers: Case report and published work review. J Dermatol. 2018;45:1195-8.
- [CrossRef] [PubMed] [Google Scholar]
- False “melanocytic” parameters shown by pigmented seborrheic keratoses: A finding which is not uncommon in dermoscopy. Dermatol Surg. 2002;28:776-9.
- [CrossRef] [PubMed] [Google Scholar]
- Pigmented wart due to human papilloma virus type 60 showing parallel ridge pattern in dermoscopy. Eur J Dermatol. 2009;19:643-4.
- [CrossRef] [PubMed] [Google Scholar]
- Key points in dermoscopic differentiation between early acral melanoma and acral nevus. J Dermatol. 2011;38:25-34.
- [CrossRef] [PubMed] [Google Scholar]




