Translate this page into:
Pigmented Bowen's disease with prominent amyloid deposition on the eyelid
2 Department of Dermatology,Anatomical Pathology, Division of Pathophysiological and Experimental Pathology, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan
3 Department of Dermatology, Pathology, Division of Pathophysiological and Experimental Pathology, Graduate School of Medical Sciences, Kyushu University, Japan
Correspondence Address:
Takamichi Ito
Department of Dermatology, Graduate School of Medical Sciences, Kyushu University, 3-1-1 Maidashi, Higashiku, Fukuoka 812-8582
Japan
| How to cite this article: Ito T, Wada M, Kuma Y, Kido-Nakahara M, Yamada Y, Okano S, Oda Y, Furue M. Pigmented Bowen's disease with prominent amyloid deposition on the eyelid . Indian J Dermatol Venereol Leprol 2014;80:558-560 |
Sir,
Bowen′s disease is a clinical expression of squamous cell carcinoma in situ of the skin. It typically arises in sun-exposed areas of older, fair-skinned individuals. [1] While most cases of Bowen′s disease in the fair-skinned develop as a non-pigmented pink macule, pigmented variants can occur, especially in the anogenital area; pigmented lesions on the eyelid are rather rare. Herein, we present a case of pigmented Bowen′s disease that showed an unusual appearance clinically and dermoscopically.
A 45-year-old Japanese man presented with a two-year history of a brown macule on the right lower eyelid. Physical examination revealed that the macule was 5 mm in size and had an irregular border and slightly papillomatous surface [Figure - 1]a. Dermoscopy showed a brain-like brown structure (arrow) without obvious vessel structure or scaly surface. Small pale-pink patches were arranged in part of the macule in a flower-like fashion (circle) [Figure - 1]b. We surgically resected it after the diagnosis of Bowen′s disease was made by punch biopsy. Histopathologically, the full thickness of the epidermis had been replaced by atypical keratinocytes with occasional clumping and dyskeratotic cells. Mild chronic inflammatory cells were observed in the dermis. Of note, abundant Dylon staining-positive amorphous deposits were found in the upper to mid-dermis [Figure - 1]c-e. These deposits showed green birefringence with polarized light and were weakly positive for Cytokeratin AE 1/3, findings that were consistent with secondary localized cutaneous amyloidosis.
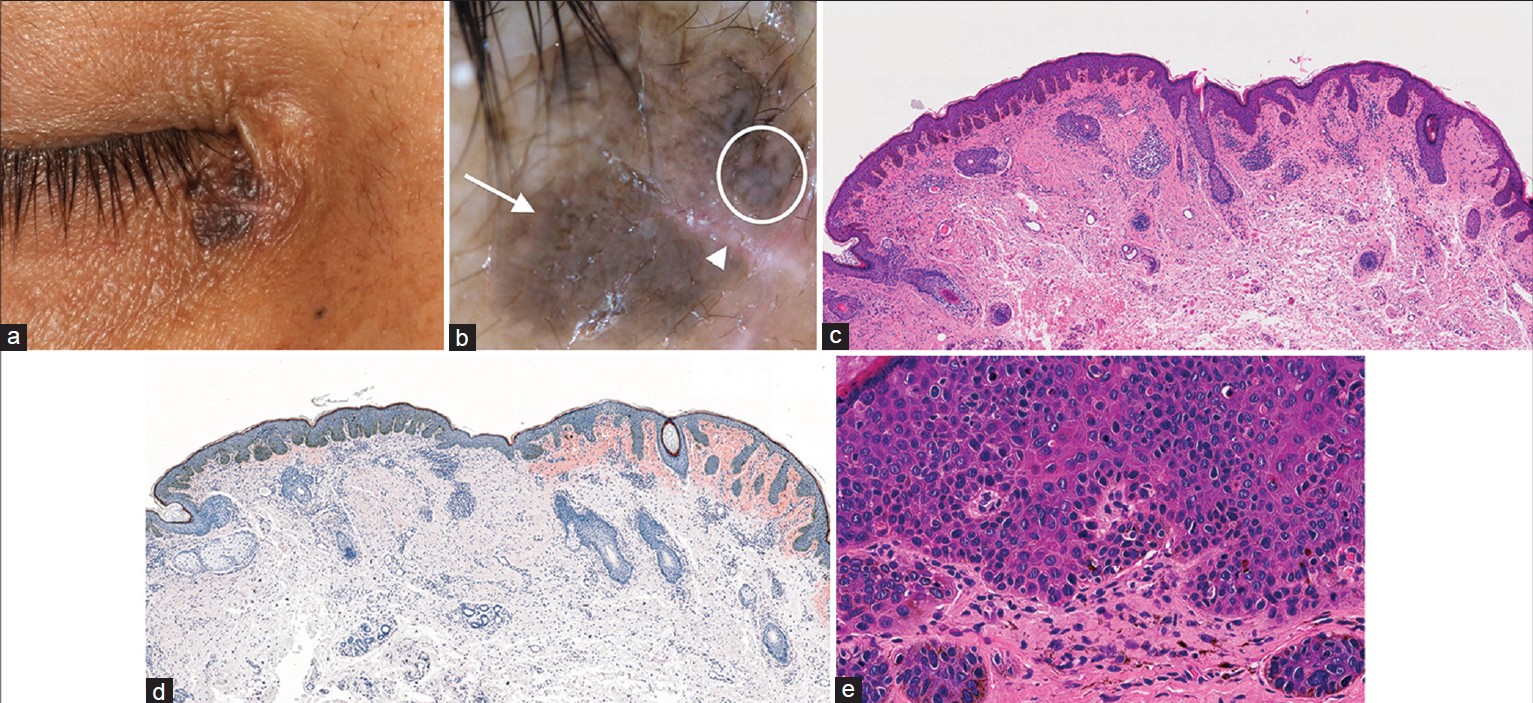 |
| Figure 1: (a) A brown plaque on the right lower eyelid. (b) Dermoscopy. A brain-like brown structure (arrow) and small pale-pink patches arranged in a fl ower-like fashion (circle). An arrowhead indicates a biopsy scar. (c, d) Full thickness of the epidermis replaced by atypical keratinocytes, mild chronic inflammatory cells and amyloid deposition in the dermis. The epidermis on the left side shows relatively regular acanthosis by atypical keratinocytes and scarce amyloid deposition. The right side also shows Bowen's disease, with irregularly elongated rate ridges, abundant amyloid deposition and underlying infl ammatory cell infi ltrates. c: H and E staining ×20; d: Dylon staining ×20, (e) High-power view of the specimen reveals atypical keratinocytes, occasional clumping cells and dyskeratotic cells |
Bowen′s disease is a superficial variant of cutaneous squamous cell carcinoma that occasionally develops into an invasive squamous cell carcinoma with an aggressive course; accurate diagnosis and appropriate treatment are necessary. It usually presents as an asymptomatic well-defined erythematous scaly plaque and making a correct diagnosis is generally easy; however, in some cases such as the pigmented variant, diagnosis may be a challenge. Only 1.7%-5.5% of cases in the fair-skinned are pigmented, and they are often misdiagnosed as seborrheic keratosis or various melanocytic lesions. [2],[3]
Dermoscopy is now applied to various skin lesions and its potential to improve the diagnostic accuracy has been acknowledged. Typical dermoscopic features of non-pigmented Bowen′s disease include glomerular vessels and surface scales. [4] In contrast, according to a detailed study on dermoscopy of the pigmented variant, a linear arrangement of brown or gray dots and coiled vessels represent clues to the diagnosis. [3] However, none of these findings was apparent in our patient which made it difficult to reach a diagnosis. In our case, there was dense pigmentation in the basal layer, incontinence of pigment in the papillary dermis, and prominent amyloid deposition in both the papillary and the reticular dermis. The brain-like lesion on dermoscopy (arrow in [Figure - 1]b) accorded with the lesion histopathologically showing a thickened epidermis and marked basal pigmentation (left part of [Figure - 1]c and d). It is likely that the thick epidermis and pigmentation obscured the underlying vessel structure. The flower-like patches, indicated by the circle in [Figure - 1]b, may reflect irregularly elongated rete ridges with basal pigmentation and underlying amyloid deposition (right part of [Figure - 1]c and d). Chuang et al. have reported a homogeneous white structure ("central hub") surrounded by radiating pigmentation as a specific dermoscopic feature of cutaneous amyloidosis. [5] Our finding of flower-like patch may correspond to grouped central hubs.
Amyloid deposition in Bowen′s disease is well known and the amyloid is considered to be derived from cytokeratin. A significant quantity of amyloid was deposited relatively deeply in the dermis in our patient, and the amyloid continued to the bottom of the lesion, giving a smooth contour overall. We speculate that the amyloid deposits were vestiges of tumor cell regression by host reaction. This hypothesis seems to be supported by lymphocytic infiltrates in the dermis and around the amyloid foci.
ACKNOWLEDGMENT
The authors thank Ms. Yuka Eguchi for her technical support with the immunostaining.
| 1. |
Weedon D. Tumor of the epidermis. In: Weedon D, editor. Weedon's Skin Pathology. Philadelphia: Churchill Livingstone Elsevier; 2010. p. 679-81.
[Google Scholar]
|
| 2. |
Ragi G, Turner MS, Klein LE, Stoll HL Jr. Pigmented Bowen's disease and review of 420 Bowen's disease lesions. J Dermatol Surg Oncol 1988;14:765-9.
[Google Scholar]
|
| 3. |
Cameron A, Rosendahl C, Tschandl P, Riedl E, Kittler H. Dermatoscopy of pigmented Bowen's disease. J Am Acad Dermatol 2010;62:597-604.
[Google Scholar]
|
| 4. |
Zalaudek I, Kreusch J, Giacomel J, Ferrara G, Catricalà C, Argenziano G. How to diagnose nonpigmented skin tumors: A review of vascular structures seen with dermoscopy: Part II. Nonmelanocytic skin tumors. J Am Acad Dermatol 2010;63:377-86.
[Google Scholar]
|
| 5. |
Chuang YY, Lee DD, Lin CS, Chang YJ, Tanaka M, Chang YT, et al. Characteristic dermoscopic features of primary cutaneous amyloidosis: A study of 35 cases. Br J Dermatol 2012;167:548-54.
[Google Scholar]
|
Fulltext Views
2,913
PDF downloads
1,679





![[Figure - 1]](#fig_ijdvl_2014_80_6_558_144204_u1.jpg){kind=link}