
Translate this page into:
Pigmented nodular lesion below eyelid in a retro positive patient
Corresponding author: Dr. Likhitha Reddy C, Department of Plastic Surgery, AIIMS, Mangalagiri, Guntur, India. drlikhitha.pls@aiimsmangalagiri.edu.in
-
Received: ,
Accepted: ,
How to cite this article: Rajagopal P, C LR, Gopinath H, Shankaralingappa A. Pigmented nodular lesion below eyelid in a retro positive patient. Indian J Dermatol Venereol Leprol. doi: 10.25259/IJDVL_1464_2024
A 39-year-old lady presented to the outpatient department with complaints of an itchy black nodule below her right eyes. She reported that the lesion had slowly grown to its present size over the last one year. She was HIV positive and was on highly active antiretroviral therapy. She did not report weight loss, fever, or any significant past or family history. On clinical examination, a solitary pigmented dome-shaped exophytic papule (1.2×1.0×0.8 cm in size) with a keratotic center was seen below the right eyelid [Figure 1]. The lesion was excised and sent for histopathological evaluation. Histopathology revealed an exo- and endophytic cup-shaped lesion lined by squamous epithelium with marked hyperkeratosis, parakeratosis, filiform papillomatosis, and lobular configuration at the epithelial stromal interface [Figure 2a]. The lobules had peripheral basaloid and central squamous cells with the presence of a few squamous eddies and microvesicle formation [Figure 2b]. Melanin deposition and increased dendritic melanocytes were also seen [Figure 2c]. No ragged edges of squamous epithelium, overt nuclear atypia, or glassy eosinophilic cytoplasm were seen.

- Hyperpigmented dome-shaped lesion with central keratotic crust near the right lower eyelid.
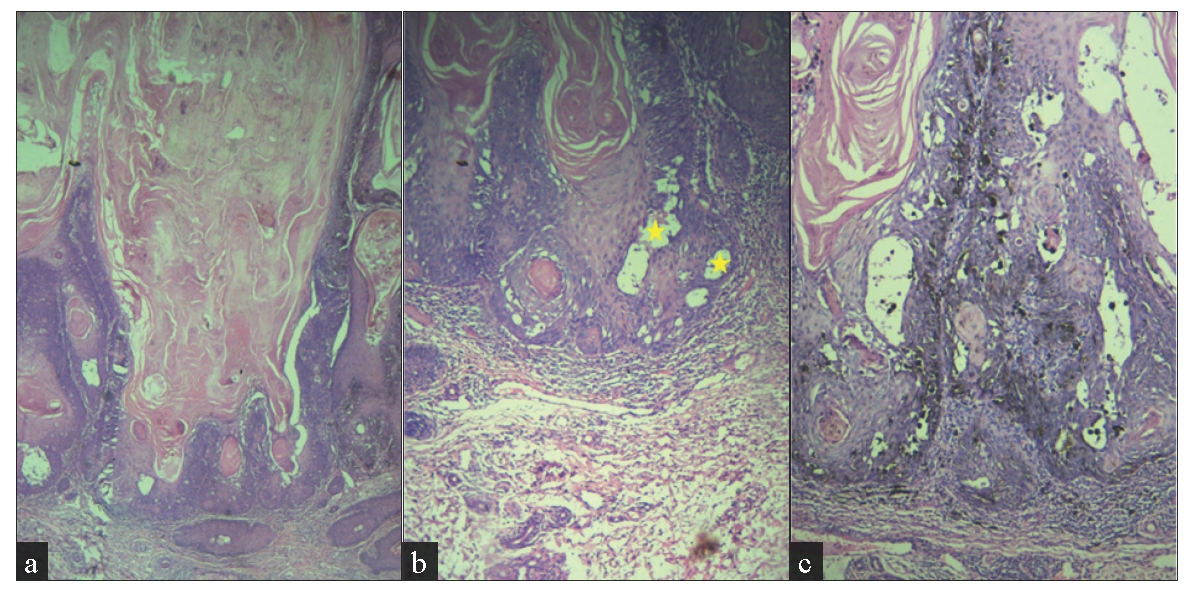
- (a) Exo and endophytic proliferative squamous lesion with a central cup-shaped area filled with hyperkeratotic, parakeratinised material with blunt edges at epithelial-stromal interface (Haematoxylin and eosin, 40x), (b) microvesicles (stars) and squamous eddies (400x) and (c) increased dendritic melanocytes (100x).
Question
What is your diagnosis?
Diagnosis
Pigmented inverted follicular keratosis
Treatment
The lesion was already excised in toto with margins considering a possibility of malignancy clinically.
Discussion
Inverted follicular keratosis is a benign tumour of follicular infundibulum. It usually presents as a solitary skin-coloured papule or nodule, usually on the face and eyelid.1 Clinically, a nodular dome-shaped lesion on the face raises the differential diagnosis of basal cell carcinoma, keratoacanthoma, squamous cell carcinoma, and at times malignant melanoma, seborrheic keratosis, and verruca vulgaris.2–4 Knowledge of the differential diagnostic possibilities could enable the clinician to make an appropriate decision; however, at times it can be difficult to differentiate a benign from a malignant lesion.
Histopathological examination is mandatory in arriving at a correct diagnosis. Benign and malignant neoplasms can create diagnostic confusion with inverted follicular keratosis not only clinically but also histopathologically.1–3 The differential diagnosis1-4 of inverted follicular keratosis is given in Table 1. Even though, in this case, histologically the cup-shaped nature of the lesion created a diagnostic confusion with keratoacanthoma, the endophytic extension, blunt edge interface with stroma, squamous eddies, and microvesicles in the absence of glassy eosinophilic cytoplasm and ragged infiltrative edges guided us to the diagnosis of pigmented inverted follicular keratosis.
| S. No | Histopathology features | Inverted follicular keratosis | Keratoacanthoma | Seborrheic keratosis | Verruca vulgaris | Squamous cell carcinoma | Basal cell carcinoma |
|---|---|---|---|---|---|---|---|
| 1 | Nature of lesion | Exo- and endophytic | Usually endophytic | Exophytic | Exophytic | Ulcero-proliferative | Nodular |
| 2 | Koliocytes | Can be seen | Absent | Absent | Present | Usually absent | Absent |
| 3 | Chunky hypergranulosis | Can be seen | Absent | Absent | Present | Usually absent | Absent |
| 4 | Epithelial stromal interface | Pushing with blunt edges | Can be infiltrative | Pushing | Pushing | Infiltrative | Pushing |
| 5 | Glassy eosinophilic squamous cells | Absent | Present | Absent | Absent | Absent | Absent |
| 6 | Mitosis | Not uncommon in basal layers | Common throughout the epithelium | Absent or limited to basal layer | Absent or limited to basal layer | Common throughout the epithelium | Common throughout the epithelium |
| 7 | Atypical mitosis | Absent | Present | Absent | Absent | Present | Present |
| 8 | Cellular composition | Peripheral basaloid and central squamous cells | Squamous cells with glassy eosinophilic cytoplasm | Basaloid cells | Squamous cells | Atypical squamous cells | Basaloid cells with peripheral palisading |
| 8 | Microcysts in epithelium | Common | Absent | Absent | Absent | Absent | Absent |
Inverted follicular keratosis can mimic other tumours even on dermoscopy. Dermoscopic features include a keratoacanthoma-like pattern with a central white amorphous area surrounded radially by hairpin vessels and a white halo and central yellow-white amorphous areas surrounded radially by hairpin vessels. Less common features include milky red globules, arborising vessels, linear irregular vessels and corkscrew vessels.1,2,5
With respect to the HIV positive status of the patient, certain skin lesions may present differently or appear more frequently due to the effects of immunosuppression. While inverted follicular keratosis is not specifically linked to retroviral infection, it’s important to differentiate inverted follicular keratosis from other lesions, including more serious conditions like squamous cell carcinoma, Kaposi’s sarcoma or viral warts. A biopsy is needed to confirm the diagnosis, particularly in the context of immunosuppression.
Inverted follicular keratosis lesions are usually cured by surgical excision.5 In our case, complete excision with 5 mm margin was done since pigmented basal cell carcinoma was in the differential diagnoses.
Inverted follicular keratosis is a relatively rare benign adnexal tumour of hair follicle origin. Clinical diagnosis of inverted follicular keratosis is difficult and it may be misdiagnosed as other malignant conditions such as basal cell carcinoma. More awareness about this entity is needed and it should be considered as one of the differentials for pigmented nodular dome-shaped lesions in the face.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of AI-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Inverted follicular keratosis: Dermoscopic and reflectance confocal microscopic features. Dermatology. 2013;227:62-6.
- [CrossRef] [PubMed] [Google Scholar]
- A rare case of inverted follicular keratosis in an elderly male: Dermoscopic and histopathological overview with therapeutic response to imiquimod. Indian J Dermatol Venereol Leprol. 2021;87:455.
- [CrossRef] [PubMed] [Google Scholar]
- Pigmented inverted follicular keratosis masquerading as basal cell carcinoma. Indian Dermatol Online J. 2022;13:669-71.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Two distinct lesions of inverted follicular keratosis of the scalp: A case report. Cureus. 2022;14:e31055.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Dermoscopy of inverted follicular keratosis: Study of 12 cases. Clin Exp Dermatol. 2016;41:468-73.
- [CrossRef] [PubMed] [Google Scholar]




