Translate this page into:
Pigmented papule on the volar aspect of left middle finger
Correspondence Address:
Tao Qu
No. 1, Shuaifuyuan, Dongcheng District, Beijing
China
| How to cite this article: Jia QN, Fang K, Qu T. Pigmented papule on the volar aspect of left middle finger. Indian J Dermatol Venereol Leprol 2020;86:743-746 |
Clinical History
A 43-year-old woman presented to Peking Union Medical College Hospital, Beijing, China with a black, firm papule on the volar aspect of the left middle finger, present since 2 years. Physical examination revealed a pigmented, elevated, verrucous papule of size 2mm [Figure - 1]. Systemic examination findings were unremarkable. Histopathology revealed proliferation of basaloid cells extending from the basal epidermis into the dermis [Figure - 2]a. The cuboidal tumor cells were characterized by scant eosinophilic cytoplasm and small monomorphous nuclei [Figure - 2]b. The tumor grew downward in broad anastomosing bands, with highly fibrovascularized stroma [Figure - 2]b. Parakeratosis and crust were present in the overlying epidermis. Dendritic melanocytes and abundant melanin deposition were also observed throughout the tumor. There was no evidence of peripheral palisading of nuclei or mucinous stroma. Immunohistochemical staining with carcinoembryonic antigen and epithelial membrane antigen highlighted the eccrine ductal lumina [Figure - 2]c and [Figure - 2]d. Immunohistochemical staining with Melan-A was positive in dendritic melanocytes [Figure - 2]e. The patient underwent surgical excision and there was no recurrence in the 9-month follow-up period.
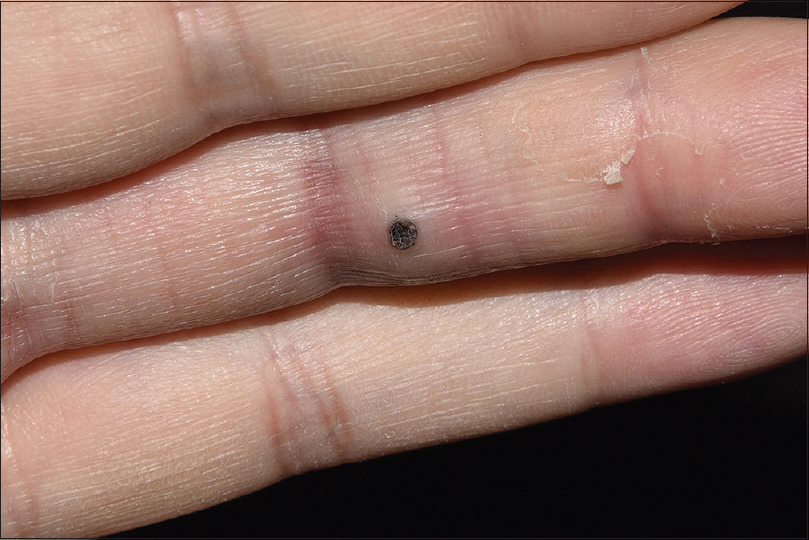 |
| Figure 1: Pigmented, elevated, verrucous papule on the left middle finger |
 |
What is Your Diagnosis?
Answer
Pigmented eccrine poroma.
Discussion
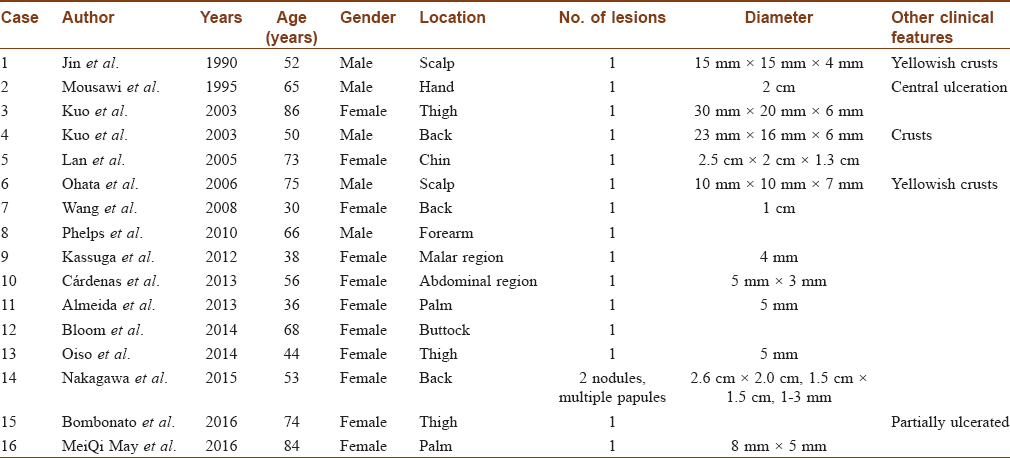
Eccrine poroma is an adnexal tumor of the terminal eccrine duct. It usually presents as a skin-colored or reddish papule, plaque, or nodule. Eccrine poroma can form anywhere where eccrine glands are present and is most commonly located on the acral sites. However, the rare pigmented variant has a predilection for the non-acral sites. We searched PubMed (1986–2016) for reports of the pigmented variant and reviewed the sixteen available cases. Only 3 (18.8%) cases were located in palmoplantar areas [Table - 1]. The average age of patients was 59 years (ranging from 30 to 86 years). The male-to-female ratio was 0.45, showing a higher prevalence in female patients; while eccrine poroma has no gender predilection. Moreover, this case is exceptional for its location and maybe clinically confused with cutaneous melanoma. Other differential diagnoses include pigmented basal cell carcinoma, verruca vulgaris, seborrheic keratosis and hidradenoma.
Histopathology is the gold standard for the diagnosis of pigmented eccrine poroma. The characteristics of this tumor are monomorphic basaloid cells with poroid differentiation and a highly fibrovascularized stroma. It is also characterized by the presence of melanin and proliferation of melanocytes. Verruca vulgaris exhibits digitate epidermal hyperplasia and koilocytosis in granular layer and dilated capillaries in papillae. Cutaneous melanoma is poorly circumscribed and is characterized by nests of atypical melanocytes with pleomorphic nuclei and mitotic figures. Basaloid cells are also present in seborrheic keratosis and basal cell carcinoma. In contrast to eccrine poroma, seborrheic keratosis may present horn cysts without ductal differentiation. In basal cell carcinoma, basaloid cells form nests with characteristic peripheral palisading and retraction artifacts. Hidradenoma is characterized by larger cells and nuclei without broad-based connection to the epidermis or the granulation tissue-like stroma.
Compared with the nonpigmented eccrine poroma of the palms, this pigmented case had evident proliferation of melanocytes [Figure - 2]e and [Figure - 2]f. Given the low density of melanocytes in palmoplantar region, there are several hypotheses of melanocyte proliferation. Melanocytes may be activated by endothelin-1, which promotes proliferation, survival, and migration of melanocytes.[1] Another hypothesis supports the migration of melanocytes from nearby epidermis or hair follicles to the lesion.[2]
Pigmented variant is extremely rare on the palmoplantar region, which is the most common site of eccrine poroma. Meanwhile, the presence of melanin and melanocytes do not always produce clinically visible pigmentation.[3] There are some explanations of these remarkable phenomena. One is that palmoplantar fibroblasts express high levels of dickkopf1, which inhibits growth and survival of melanocytes and production of melanin.[4] Another one is that fibronectin, which promotes melanocyte proliferation, differentiation, and migration, is expressed in lower levels in palmoplantar region.[5] This may suggest that melanocytes proliferate and survive poorly in acral sites, thus explaining the unusual occurrence of pigmented eccrine poroma in acral sites.
As a benign tumor, therapeutic options in the management of eccrine poroma include shaving, electrosurgical destruction and surgical excision. However, in consideration of the possible malignant transformation and recurrence, complete surgical excision is advocated.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understand that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Chiu HH, Chen PH, Wu CS, Chen GS, Tsai KB, Wen CH, et al. Origin of poroid hidradenoma and pigmentation mechanism of eccrine poroma: Critical analysis of an unique presentation. J Eur Acad Dermatol Venereol 2009;23:597-9.
[Google Scholar]
|
| 2. |
Ohata U, Hara H, Suzuki H. Pigmented eccrine poroma occurring on the scalp: Derivation of melanocytes in the tumor. Am J Dermatopathol 2006;28:138-41.
[Google Scholar]
|
| 3. |
Betti R, Bombonato C, Cerri A, Moneghini L, Abramo P, Menni S, et al. Clinically and/or histologically pigmented poromas in Caucasian patients. G Ital Dermatol Venereol 2014;149:341-6.
[Google Scholar]
|
| 4. |
Yamaguchi Y, Passeron T, Watabe H, Yasumoto K, Rouzaud F, Hoashi T, et al. The effects of dickkopf 1 on gene expression and Wnt signaling by melanocytes: Mechanisms underlying its suppression of melanocyte function and proliferation. J Invest Dermatol 2007;127:1217-25.
[Google Scholar]
|
| 5. |
Yasuda M, Miyachi Y, Ishikawa O, Takahashi K. Spatial expressions of fibronectin and integrins by human and rodent dermal fibroblasts. Br J Dermatol 2006;155:522-31.
[Google Scholar]
|
Fulltext Views
4,268
PDF downloads
2,629





![[Figure - 1]](#fig_ijdvl_2020_86_6_743_257917_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2020_86_6_743_257917_f2.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2020_86_6_743_257917_t3.jpg){kind=link}