Translate this page into:
Pilomatricoma: A tumor with hidden depths
Correspondence Address:
T Rajalakshmi
Department of Pathology, St. John's Medical College, Bangalore - 560 034
India
| How to cite this article: Simi C M, Rajalakshmi T, Correa M. Pilomatricoma: A tumor with hidden depths. Indian J Dermatol Venereol Leprol 2010;76:543-546 |
Abstract
Background: Pilomatricoma is a benign tumor of hair matrix differentiation and has been classically described as comprising of basaloid and shadow cells admixed with multinucleated giant cells and areas of calcification. However, there are a diverse range of histologic features this tumor displays that are often unrecognized. Aims: This study was undertaken to record the histopathologic features of pilomatricoma with an emphasis on the occurrence of other forms of differentiation. Methods: The study included all skin biopsy specimens over a 13-year period from 1995 to 2007 that had a histologic diagnosis of pilomatricoma. Hematoxylin and eosin-stained slides were reviewed. Results: This study included 21 cases of pilomatricoma. Supramatrical differentiation was seen in all cases and three-quarters of the cases showed matrical differentiation. Also observed in some of the cases were clear cell differentiation toward the outer root sheath, infundibular differentiation, calcification, ossification and secondary inflammation with a foreign body giant cell reaction. Epidermal induction in the form of a downward plate-like growth of the epidermis was seen in a few cases. Conclusion: Pilomatricoma, although considered a tumor of hair matrix differentiation, can show cellular evolution toward the other parts of the hair follicle, such as the outer and inner root sheaths, sebaceous and infundibular components and, therefore, can be considered a panfollicular neoplasm.Introduction
Pilomatricoma is a common benign neoplasm, which is considered to differentiate toward hair follicular cells, particularly the cortex. [1] Typically, it is said to comprise of "basaloid, eosinophilic and shadow cells" with calcification. [2] Ackerman and coworkers elaborated on pilomatricoma extensively. [3] They describe pilomatricoma as a sac of epithelium that is infundibular above and matrical and supramatrical cells along the sides and below. The authors also mention that matrical cells of pilomatricoma not only cornify as shadow cells but also differentiate according to other counterparts of a normal hair follicle, e.g. toward inner sheath and infundibulum. These features are usually not emphasized and this study is an attempt to document the range of differentiation seen in this tumor. This study was undertaken to determine the histopathological features of pilomatricoma with an emphasis on the occurrence of nonmatrical forms of differentiation.
Methods
The study included all skin biopsy specimens received at the Department of Pathology over a 13-year period from July 1995 to July 2007, which were signed out as pilomatricoma. Hematoxylin and eosin-stained sections were reviewed. The features studied were matrical cells, supramatrical cells, shadow cells, isthmic epithelium, infundibular epithelium, sebocytes, apocrine cells, calcification, ossification, melanocytes, giant cell response and granulomas. Clinical data was obtained from the patient records.
Results
Twenty-one pilomatricomas were seen in 20 patients. The age of the patients ranged from 6 years to 42 years. Most cases were seen in the 2 nd and 3 rd decade. A male preponderance (six female and 14 male patients) was noted. The arm and forearm were the most common sites involved, followed by neck, trunk, thigh, gluteal region and leg. One patient had multiple lesions (two in number). The size of the lesions ranged from 0.5 cm to 2 cm in greatest dimension.
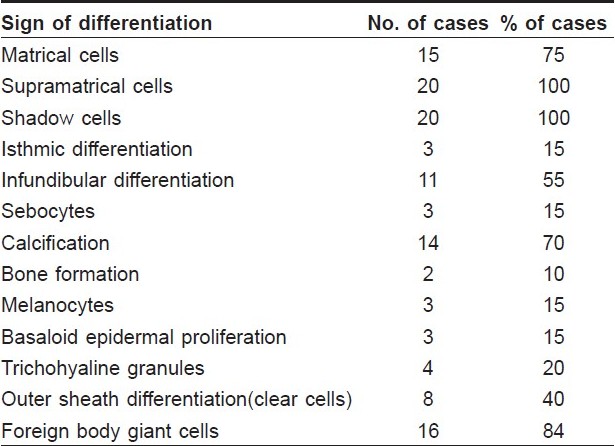
The microscopic features seen in pilomatricoma are summarized in [Table - 1]. The classic appearance of "basaloid and eosinophilic cells" was seen in all cases [Figure - 1]a, with the mature ones being composed only of eosinophilic "ghost" cells [Figure - 1]b. All the cases of pilomatricoma showed supramatrical differentiation [Figure - 2]a, i.e. cellular areas with pale staining cells having a moderate amount cytoplasm and a not very crowded appearance as compared with the areas of matrical differentiation. Matrical differentiation, as characterized by areas showing closely packed basaloid cells having round, pale staining and finely stippled nuclei with prominent nucleoli, was seen in 75% of the cases [Figure - 2]a. Clear cells, indicative of outer root sheath differentiation, was characterized by the presence of large vacuolated cells [Figure - 2]b. In three cases, sebaceous differentiation was present focally in the form of cells with a vacuolated cytoplasm and scalloped nuclei. Signs of differentiation toward the inner sheath took the form of trichohyaline granules [Figure - 2]c. Signs of infundibular differentiation (in 55% cases) included keratohyaline granules and basket woven orthokeratosis [Figure - 2]d. In 15% of the cases, the epithelium of pilomatricoma resembled that of the isthmus of a follicle, characterized by cells replete with pink cytoplasm, absence of a granular zone and a prominent, brightly eosinophilic cornified layer whose cells are arranged compactly [Figure - 2]e. Four cases showed trichohyaline granules. Melanocytes were found in three cases [Figure - 2]f. We did not see any apocrine cells.
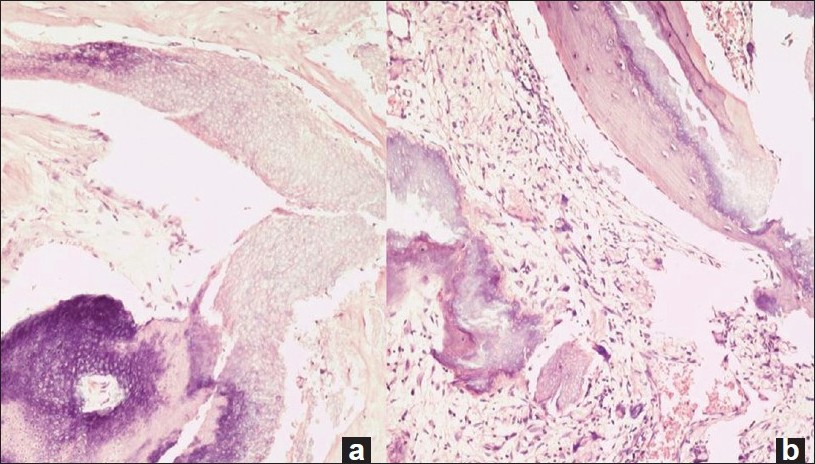 |
| Figure 1 :Pilomatricoma showing characteristic "basaloid and eosinophilic" cells (a). An older lesion with calcification, ossification and ghost cells (b) (H and E, x200) |
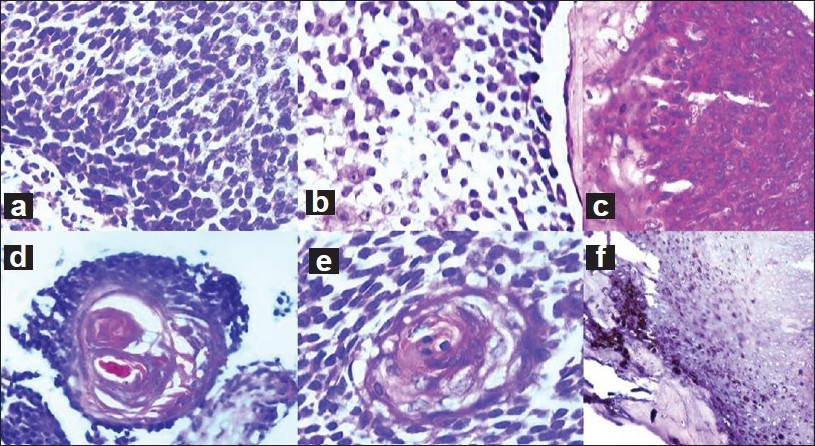 |
| Figure 2 :(a) Matrical and supramatrical cells (H and E, x400). (b) Clear cells of outer root sheath differentiation (H and E, x400). (c) Bright red trichohyaline granules, sign of inner root sheath differentiation (H and E, x400). (d) Infundibular differentiation evidenced by basket-woven orthokeratosis and keratohyaline granules (H and E, x400). (e) Cells with pink cytoplasm, absence of a granular zone and a prominent, brightly eosinophilic cornified layer, signs of isthmic differentiation (H and E, x400). (f) Melanocytes seen focally (H and E, x200) |
Basaloid epidermal proliferation in the form of a plate-like growth of the epidermis down to the dermis was noticed in three cases. Calcification and ossification were frequently seen. Foreign body reaction was common.
Discussion
Pilomatricoma is a benign neoplasm, with differentiation toward the matrix of the hair follicle, first described in 1880 by Malherbe and Chenantais as a tumor of the sebaceous glands. [4] It is most frequently seen in the 1 st and 2 nd decade. The age range of patients in this study was consistent with that of published literature. [2] Although pilomatricomas in general have a slight female predominance, we noted a male preponderance. Head, upper extremity, neck, trunk and lower extremity are affected with decreasing frequency. [2] In an Indian study by Solanki et al., the arm was the most common site involved, concordant with the current study where the lesions were predominantly located on the upper extremity. [5] Moehlenbeck et al. found multiple lesions in up to 3.5% of the cases. [6]
Pilomatricoma, although considered a tumor of hair matrical differentiation, is now believed to be a complex panfollicular neoplasm, in that it can exhibit signs of differentiation of the entire follicle. Ackerman and coworkers have described not only shadow cells that represent an aberrant attempt at hair formation but also differentiation to other parts of a hair follicle, i.e. toward the inner sheath, as evidenced by the presence of trichohyaline granules, toward the infundibulum, as evidenced by the presence of keratohyaline granules and basket-woven orthokeratosis and sometimes toward the sebaceous and isthmic epithelium.
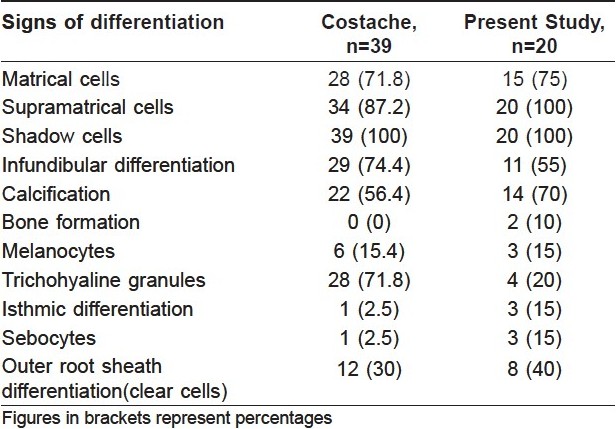
We found only one study of 39 cases by Costache that discusses these features in detail, and none from India. [7] [Table - 2] gives a comparison of our findings with that of Costache. The results are more or less concordant. We found a lower rate of infundibular differentiation. It is noteworthy that melanocytes were seen with a similar frequency in both studies. When abundant, these tumors have been termed melanocytic matricomas. Clear cells, a sign of outer root sheath differentiation, need to be distinguished from sebocytes, which not only have a fine, multivacuolated cytoplasm but also have scalloped nuclear outlines. The range of differentiation encountered is a reflection of the common embryologic origin of the folliculo-sebaceous-apocrine unit.
The reported incidence of calcification in pilomatricoma ranges from 69% to 85%, and osseous metaplasia has been described in 15% of the cases. [8] In this series, calcification was seen in 68% and ossification in 5%. Other secondary changes such as foreign body giant cell reaction, which is well documented in the literature, were common.
Another unusual feature that we incidentally noticed was basaloid proliferation of the epidermis overlying the neoplasm, forming a plate-like structure resembling follicular germinative cells. This phenomenon is often described in mesenchymal proliferations such as dermatofibroma, where the stroma induces the epidermis to behave like the surface ectoderm. [9] We do not know the reason for its occurrence in pilomatricomas, but speculate that it may be due to changes in the surrounding stroma.
To conclude, pilomatricoma, a tumor deemed to be of hair matrix differentiation, commonly shows cellular evolution toward other parts of the hair follicle such as the outer and inner root sheaths and sebaceous and infundibular components. These features are often not stressed in the literature. If one is not aware of this fascinating array of appearances, it is quite likely that the diagnosis may be missed, especially on small biopsies or needle aspirates.
| 1. |
Elder DE, Johnson BL, Elenitsas R. Lever′s Histopathology of the Skin. Philadelphia: Lippincott Williams and Wilkins; 2005.
[Google Scholar]
|
| 2. |
Hurt MA, Kaddu S, Kutzner H, Cribier B, Schulz T, Hartschuh W. Benign tunours with follicular differentiation in Pathology and Genetics of Skin: 152-163 tumours. In: LeBoit PE, Burg G, Weedon D, Sarasin A, editors. Lyon: IARC Press; 2006.
[Google Scholar]
|
| 3. |
Ackerman AB, Reddy VB, Soyer HP. Neoplasms with Follicular Differentiation. 2 nd ed. New York: Ardor Scribendi, Ltd.; 2001.
[Google Scholar]
|
| 4. |
Peterson WC Jr, Hult AM. Calcifying epithelioma of Malherbe. Arch Dermatol 1964;90:404-10.
[Google Scholar]
|
| 5. |
Solanki P, Ramzy I, Durr N, Henkes D. Pilomatrixoma. Cytologic features with differential diagnostic considerations. Arch Pathol Lab Med 1987;111:294-7.
[Google Scholar]
|
| 6. |
Moehlenbeck FW. Pilomatricoma. Arch Dermatol 1973;108:532-4.
[Google Scholar]
|
| 7. |
Costache M. Pilomatricoma - A neoplasm of panfollicular differentiation. Dermatopathology: Practical and Conceptual 2007; 13:#2. Available from: http://www.derm101.com . [last accessed on 2009 Dec 30].
[Google Scholar]
|
| 8. |
Kaddu S, Beham-Schmid C, Soyer HP, Hφdl S, Beham A, Kerl H. Extramedullary hematopoiesis in pilomatricomas. Am J Dermatopathol 1995;17:126-30.
[Google Scholar]
|
| 9. |
Ackerman AB, Boer A. Histopathologic Diagnosis of Adnexal Epithelial Neoplasms Atlas and text. New York: Ardor Scribendi; 2008. p. 203-5.
[Google Scholar]
|
Fulltext Views
4,462
PDF downloads
2,376





![[Table - 1]](#tbl_ijdvl_2010_76_5_543_69086_t1.jpg){kind=link}
![[Figure - 1]](#fig_ijdvl_2010_76_5_543_69086_f3.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2010_76_5_543_69086_f4.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2010_76_5_543_69086_t2.jpg){kind=link}