Translate this page into:
Pityriasis rosea along Blaschko's lines: A rare variant
2 JC School of Public Health, The Chinese University of Hong Kong and The Prince of Wales Hospital, Shatin, Hong Kong,
Correspondence Address:
Vijay Zawar
Skin Disease Center, Shreeram Sankul Opp. Hotel Panchavati, Vakilwadi, Nashik - 422 002, Maharashtra
India
| How to cite this article: Zawar V, Chuh A. Pityriasis rosea along Blaschko's lines: A rare variant. Indian J Dermatol Venereol Leprol 2017;83:516 |
Sir,
Several variants of pityriasis rosea are known.[1] The most important recognized associations of pityriasis rosea are primary infection and endogenous reactivation of human herpesvirus-7 and 6.[2] Failure to recognize atypical manifestations of pityriasis rosea may pose the risks of misdiagnosis, delayed diagnosis and unnecessary investigations. An early accurate diagnosis ensures the timely delivery of the most appropriate therapy.
A student, aged 20 years, suffered from sore throat, nasal congestion and generalized fatigue. He consulted a general practitioner and was prescribed a 3-day course of oral azithromycin and paracetamol. One week after the onset of his coryzal symptoms, he noted a slightly pruritic skin lesion on his right thigh. Another five days later, he noted the eruption of smaller lesions near the initial lesion.
His health had been good in the past. There was history of atopic dermatitis or psoriasis in him or his family members. The history did not substantiate allergic or irritant contact dermatitis.
Examination revealed a large and slightly pruritic plaque on the lateral aspect of his right thigh. Close examination revealed peripheral collarette scaling [Figure 1a]. There were smaller plaques and papules in the vicinity of initial plaque, affecting only his right thigh. The larger secondary lesions also revealed peripheral collarette scaling. The distribution of lesions was along an oblique arbitrary zone stretching from the region of the right anterior superior iliac spine to the medial aspect of the right thigh [Figure 1b].
 |
| Figure 1a: Collarette scaling in the first, large lesion, the herald plaque (black arrow) on the upper part of right thigh |
 |
| Figure 1b: Secondary lesions in a Blaschkoid distribution. The discrete lesions were along an oblique zone stretching from the region of the right anterior superior iliac spine to the medial aspect of the right thigh |
Our provisional diagnosis was pityriasis rosea as the rash fulfilled the diagnostic criteria of pityriasis rosea.[3] We suspected Blaschkoid pityriasis rosea, owing to the strictly unilateral presence of a single group of lesions along the linear oblique stripe. We obtained a diagram on Blaschkoid's lines and found that the distribution of lesions in our patient directly corresponded to these lines as shown color-filled in red [Figure - 2]. There were no other lesions on the rest of the skin. Mucosal surfaces were not involved. General and systemic examination revealed no abnormality.
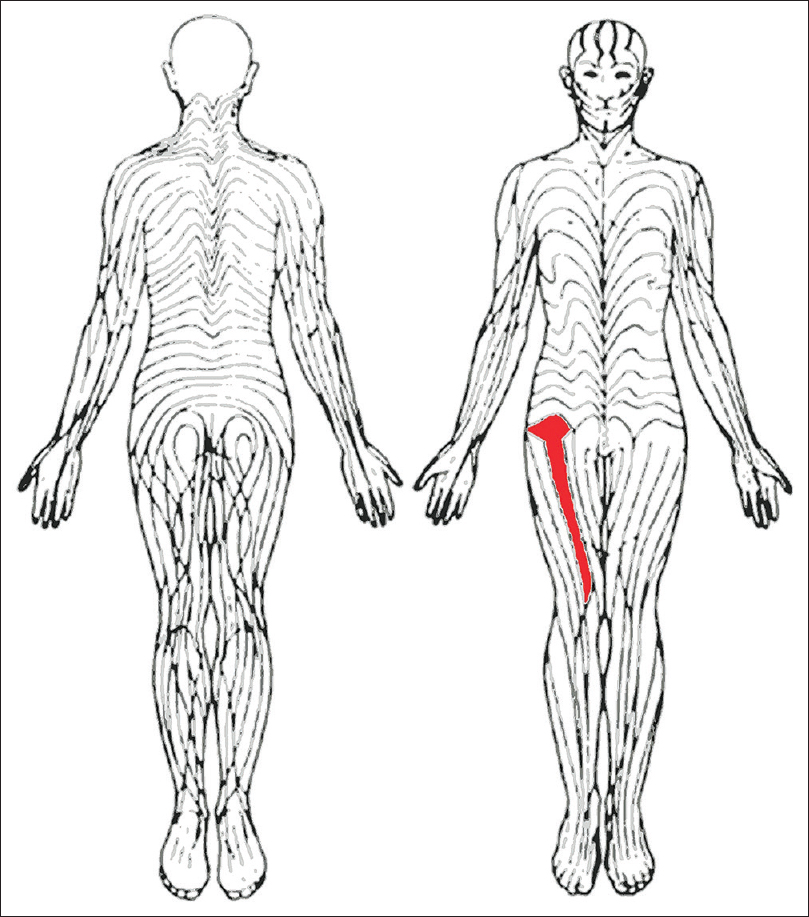 |
| Figure 2: Classical Blaschko's lines on the anterior aspect of the thigh color-filled in red, matching with affected areas in our patient |
Apart from marginal lymphocytosis, all other investigations were negative including venereal disease research laboratory, human immunodeficiency virus antibodies, antistreptolysin O titer and potassium hydroxide smear of skin scrapings for the detection of fungal hyphae. Biopsy from the margin of the herald patch revealed parakeratosis, epidermal spongiosis, extravasation of erythrocytes and upper dermal lymphocytic infiltrates, mainly conglomerated in the perivascular areas.
Before coming to us, he consulted a general practitioner, who prescribed a combination cream of betamethasone dipropionate and fusidic acid. Considering a tentative diagnosis of Blaschkoid pityriasis rosea, we prescribed oral roxithromycin 150 mg twice daily for 5 days, desloratadine 5 mg daily for 7 days and asked the patient to continue applying the combination twice daily. When he was reviewed a week later, progression of the lesions had stopped. After 2 weeks, complete remission of all lesions with slight postinflammatory hyperpigmentation was noted.
In our patient, only one group of lesions was observed and the distribution of the rash was strictly unilateral, characteristically following the Blaschko's lines. This distribution of lesions was clinically different from segmental pityriasis rosea or purely linear or classic localized pityriasis rosea.
Blaschko-linear distribution in different diseases is hypothesized to be due to unmasking of tolerance or susceptibility of keratinocytes to the underlying disease. A group or a segment of mutated keratinocytes that migrated during cell line alignment in the embryonic stage interact with external triggers, causing these keratinocytes to react and to manifest disease in the region concerned.
Blaschkoid pityriasis rosea appears to be extremely rare. We were able to find only one previous report.[4] The patient was a 42-year-old woman who developed pityriasis rosea on her left leg following an episode of pharyngitis. Other clinical manifestations were the same as in classical pityriasis rosea.
The mechanism for the development of Blaschkoid pityriasis rosea is unknown. Ang and Tay postulated that Blaschkoid pityriasis rosea is due to an abnormal response of a susceptible clone of keratinocytes, in a patient with genetic mosaicism, to an infectious stimulus. We largely agree with this hypothesis. The etiology of pityriasis rosea is believed to be related to human herpesvirus infections, particularly endogenous reactivation, of human herpesvirus-6 or human herpesvirus-7.[2] As not all patients with pityriasis rosea have virological evidence of endogenous reactivation or primary infection of human herpesvirus-7 or -6, pityriasis rosea may best be regarded as a paraviral exanthem rather than a viral exanthem.[5]
Owing to limitations in resources, we were unable to arrange virological studies such as polymerase chain reaction to detect human herpesvirus-7 and -6 deoxyribonucleic acid in lesional skin, plasma and peripheral blood mononuclear cells and serology for acute and convalescent sera to be measured in parallel for human herpesvirus-7 and -6 Immunoglobulin G titers. We, therefore, have no information regarding the association of human herpesvirus-7 and -6 infections and Blaschkoid pityriasis rosea in our patient.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Zawar V, Chuh A. Follicular pityriasis rosea. A case report and a new classification of clinical variants of the disease. J Dermatol Case Rep 2012;6:36-9.
[Google Scholar]
|
| 2. |
Drago F, Broccolo F, Javor S, Drago F, Rebora A, Parodi A. Evidence of human herpesvirus-6 and -7 reactivation in miscarrying women with pityriasis rosea. J Am Acad Dermatol 2014;71:198-9.
[Google Scholar]
|
| 3. |
Zawar V, Chuh A. Applicability of proposed diagnostic criteria of pityriasis rosea: Results of a prospective case-control study in India. Indian J Dermatol 2013;58:439-42.
[Google Scholar]
|
| 4. |
Ang CC, Tay YK. Blaschkoid pityriasis rosea. J Am Acad Dermatol 2009;61:906-8.
[Google Scholar]
|
| 5. |
Lipsker D, Saurat JH. A new concept: Paraviral eruptions. Dermatology 2005;211:309-11.
[Google Scholar]
|
Fulltext Views
4,227
PDF downloads
2,281





![[Figure - 2]](#fig_ijdvl_2017_83_4_516_193618_f2.jpg){kind=link}