Translate this page into:
Plantar erythema nodosum associated with granulomatous mastitis
Correspondence Address:
Mualla Polat
Department of Dermatology, Faculty of Medicine, Abant Izzet Baysal University, 14280 Golkoy-Bolu
Turkey
| How to cite this article: Polat M, Kaya H. Plantar erythema nodosum associated with granulomatous mastitis. Indian J Dermatol Venereol Leprol 2016;82:202-204 |
Sir,
Granulomatous mastitis is a rare benign breast disease that has clinical and radiological findings similar to those of breast cancer. Although its etiology is unclear, it commonly coexists with Wegener′s granulomatosis, sarcoidosis, diabetes mellitus, leprosy, and connective tissue disorders. It is rarely reported in association with erythema nodosum. [1],[2],[3]
Erythema nodosum is a reactive dermatosis with inflammation of the subcutaneous fat. It typically presents as an acute eruption of erythematous, tender subcutaneous nodules over the pretibial areas. Plantar erythema nodosum is rare and is usually seen in children or people with systemic diseases such as Crohn′s disease, Takayasu′s arteritis and after treatment with infliximab. [4],[5] We were unable to find any previous reports of plantar erythema nodosum associated with granulomatous mastitis.
A 30-year-old female presented to the dermatology outpatient clinic of Abant Izzet Baysal University Hospital in Turkey with a firm, painful lump in her left breast for 4 weeks. She had also been complaining of swelling of the soles of her feet for 2 weeks. She was a non-smoker and had no history of fever, night sweats, weight loss or hemoptysis. Examination revealed red, tender subcutaneous nodules on the soles of her feet [Figure - 1]a and a firm, tender, 5 × 2 cm indurated lump in the left breast. There was no lymphadenopathy and abdominal ultrasonography was normal. Test results revealed an erythrocyte sedimentation rate of 59 mm/h and C-reactive protein of 66.2 mg/L. Serum immunoglobulins and complement were normal and autoantibodies were negative. A biopsy specimen from her foot revealed mononuclear cell infiltration comprising of histiocytes, lymphocytes, rare eosinophils and slightly increased fibrous tissue within the septae of the subcutaneous fat [Figure - 1]b. Fine-needle aspiration biopsy of the breast mass revealed a granuloma with multinucleated Langerhans giant cells, neutrophils, small lymphocytes and epithelioid cells predominantly associated with the breast lobules [Figure - 2]. Bacterial, fungal and mycobacterial cultures of the aspirated specimen were negative. Chest X-ray was normal and a Mantoux test was negative. A diagnosis of erythema nodosum and granulomatous mastitis was made. Total excision of the breast lump was performed. The patient did not receive any antibiotics or antitubercular treatment prior to surgery. The erythema nodosum disappeared within 1 week after surgery without treatment. No recurrence has been noted after 10 months.
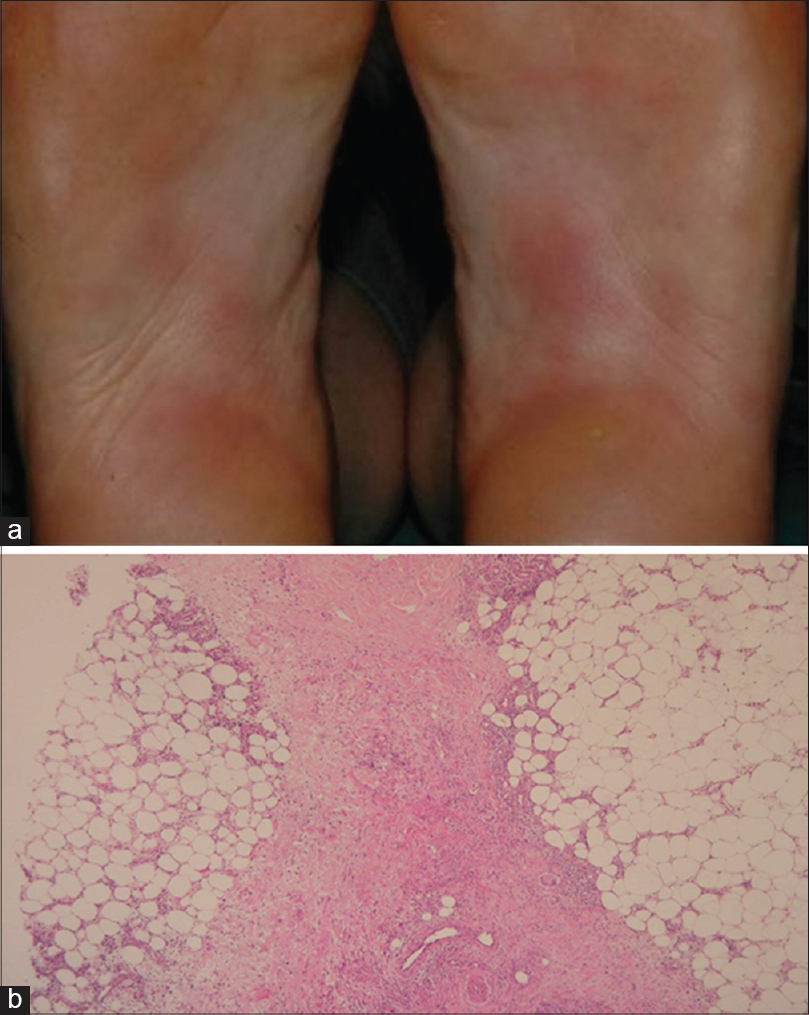 |
| Figure 1: (a) Multiple erythematous nodules on the plantar aspect of the foot. (b) Mononuclear cell infiltration within the septa of subcutaneous fat tissue (H and E, ×20) |
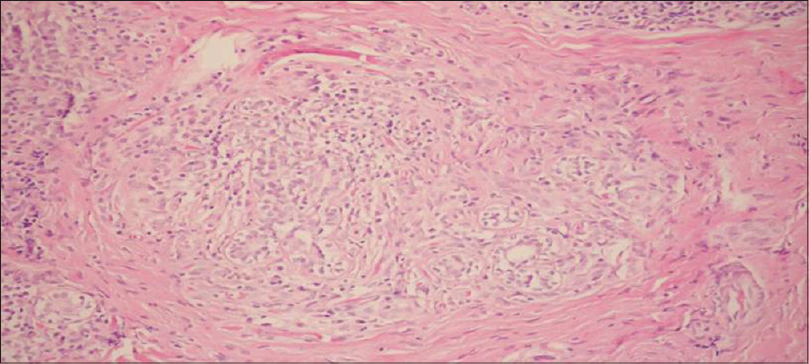 |
| Figure 2: Granulomatous microabscesses in the lumen of the breast ducts and periductal region consisting of neutrophils and epithelioid histiocytes with partial giant cell formation (H and E, ×20) |
Our patient displayed the typical clinical profile of idiopathic granulomatous mastitis as described by Kessler and Wolloch, namely the development of a very hard, painful breast lump. [1] The histological features of lymphocytes and epithelioid cells predominantly associated with the breast lobules were also typical. [1],[6]
Plantar nodular erythema is rare. Some authors have interpreted plantar nodular erythema as erythema nodosum, others as plantar eccrine hidradenitis based on histological grounds and some as unconfirmed trauma-induced change (dancing or pressure urticaria). [4],[5]
Hern and Schwayder reported the first case of erythema nodosum localized to the plantar surfaces, [4] followed by other reports. Histological confirmation was reported in only some of the cases. Conditions associated with plantar nodular erythema included increased antistreptolysin O titers, positive IgM for rubella and Mycoplasma, and ongoing infections with group A Streptococcus, Yersinia enterocolitica, and Mycobacterium tuberculosis. [5]
Granulomatous mastitis with erythema nodosum has rarely been reported in the English-language medical literature. [3],[5] This association was first reported by Adams in 1987. [3] It was associated with postpartum altered immune status; other granulomatous diseases including tuberculosis and sarcoidosis were excluded.
| 1. |
Kessler E, Wolloch Y. Granulomatous mastitis: A lesion clinically simulating carcinoma. Am J ClinPathol 1972;58:642-6.
[Google Scholar]
|
| 2. |
Pandhi D, Verma P, Sharma S, Dhawan AK. Borderline -lepromatous leprosy manifesting as granulomatous mastitis. Lepr Rev 2012;83:202-4.
[Google Scholar]
|
| 3. |
Adams DH, Hubscher SG, Scot DG. Granulomatous mastitis−A rare cause of erythema nodosum. Postgrad Med J 1987;63:581-2.
[Google Scholar]
|
| 4. |
Hern AE, Shwayder TA. Unilateral plantar erythema nodosum. J Am Acad Dermatol 1992;26:259-60.
[Google Scholar]
|
| 5. |
Sanchez-Viera M, Lecona M, Soto-Melo J. Plantar erythema nodosum of childhood. J Am Acad Dermatol 1993;29:284.
[Google Scholar]
|
| 6. |
Al-Khaffaf BH, Shanks JH, Bundred N. Erythema nodosum- An extramammary manifestation of granulomatous mastitis. Breast J 2006;12:569-70.
[Google Scholar]
|
Fulltext Views
5,439
PDF downloads
3,204





![[Figure - 1]](#fig_ijdvl_2016_82_2_202_164219_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2016_82_2_202_164219_f2.jpg){kind=link}