Translate this page into:
Pleomorphic hyalinizing angiectatic tumor of soft parts with unusual lipoma-like clinical morphology
2 Alpha Medical Patológia, Slovak Academy of Sciences, Bratislava, Slovakia
3 Cytopathos Ltd, Laboratory of Diagnostic Pathology and Cytology, Bratislava, Slovakia
4 Institute of Molecular Biology, Slovak Academy of Sciences, Bratislava, Slovakia
Correspondence Address:
Juraj Majtan
Institute of Molecular Biology, Slovak Academy of Sciences, Dubravska Cesta 21, 845 06, Bratislava
Slovakia
| How to cite this article: Szep Z, Majernikova A, Rychly B, Majtan J. Pleomorphic hyalinizing angiectatic tumor of soft parts with unusual lipoma-like clinical morphology. Indian J Dermatol Venereol Leprol 2018;84:619-621 |
Sir,
A 63-year-old woman presented with a solitary, asymptomatic, subcutaneous swelling in the medial part of the left crura of seven months duration. Examination revealed a nodule which was 4 cm × 4 cm in size, skin-colored, partially mobile, relatively well-demarcated and non-tender [Figure - 1]. The patient did not show any systemic symptoms or regional lymphadenopathy. A provisional clinical diagnosis of lipoma was made. The nodule was completely removed surgically with healthy tissue margins.
 |
| Figure 1: Palpable, relatively well-demarcated and slightly prominent lipoma-like lesion in the medial part of left crura |
A histological image (hematoxylin and eosin stain) revealed clusters of thin-walled, markedly dilated vessels of various calibre with fibrinous eosinophilic material in their walls [Figure - 2]. We distinguished two types of tumor cells – spindle cells arranged in bundles and round epithelioid cells with marked cellular and nuclear pleomorphism [Figure - 3]. Sporadically, intranuclear pseudoinclusions were found. Occasionally, inconspicuous erythrocyte extravasation and hemosiderin deposits were seen. Mitoses in tumor cells were not observed. The tumor was located subcutaneously with infiltrative growth into the dermis. Immunohistochemically, we observed a diffuse positivity for vimentin and CD34 and negativity for S100, SMA, desmin, EMA, HMB45 and CD31. Listed findings confirmed the diagnosis of pleomorphic hyalinizing angiectatic tumor of soft parts.
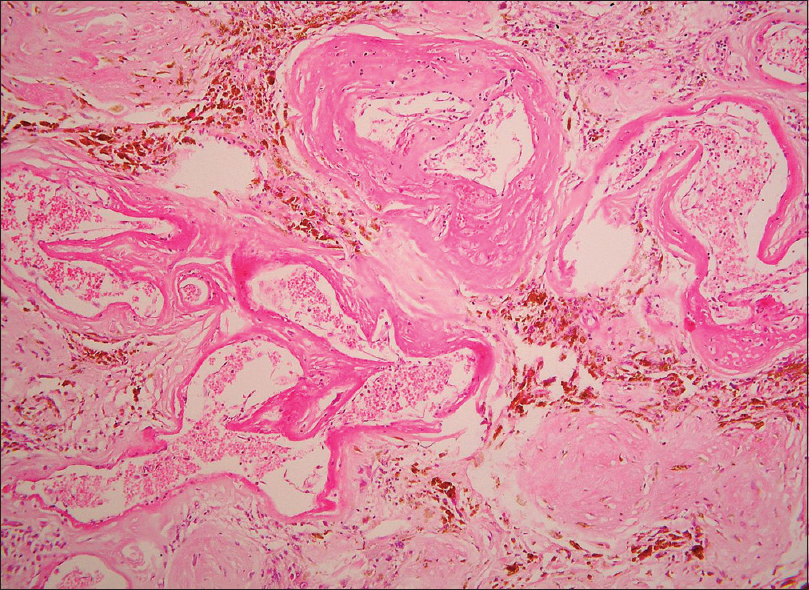 |
| Figure 2: Pleomorphic hyalinising angiectatic tumour: Clusters of thin-walled, fibrin-filled, dilated blood vessels (H and E, ×200) |
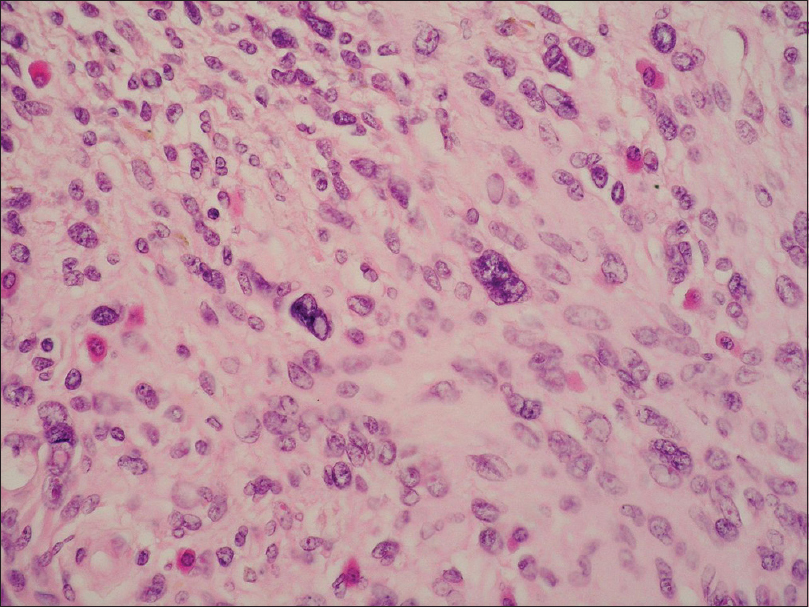 |
| Figure 3: Pleomorphic hyalinising angiectatic tumour: Spindle and pleomorphic tumour cells with nuclear atypia, no mitoses (H and E, ×400) |
The current WHO classification of soft tissue tumors considers pleomorphic hyalinizing angiectatic tumor a locally aggressive lesion of borderline behavior and uncertain differentiation.[1] Recent studies assume that pleomorphic hyalinizing angiectatic tumor, hemosideric fibrolipomatous tumor and myxoinflammatory fibroblastic sarcoma are morphological variants of the same genetically defined entity, but only the last-mentioned variant has a potential to metastasise.[1]
Pleomorphic hyalinizing angiectatic tumor occurs from the fifth to eighth decades of human life; the average age is 55 years. It is slightly predominant in female patients, at a 4:3 proportion. The tumor is frequently located in the lower extremity (63%), especially feet and ankles (27%).[1],[2]
A majority of the literature characterises the clinical presentation of pleomorphic hyalinizing angiectatic tumor as a reddish-purple or livid/violaceous lesion that may imitate hematoma, Kaposi sarcoma or other vascular lesions.[1],[2],[3] Some studies refer to it as an unspecific subcutaneous mass of clinically normal skin which resembles lipoma, Baker's cyst, desmoid tumor or other benign or malignant tumors of clinically uncharacteristic morphology.[3] Moreover, one study describes it as a combination of both clinical presentations as a hematoma-like area on the surface of a subcutaneous resistance.[4] Some authors have described it as a case of circumscribed, painful, erythematous edema located in the lower third of crura, supporting the diagnosis of fatty necrosis, erythema nodosum or pretibial myxedema.[5] Based on the findings from the literature, we may consider the spectrum of clinical manifestation of pleomorphic hyalinizing angiectatic tumor to be wider than expected. Clinically, the appearance of pleomorphic hyalinizing angiectatic tumor is non-specific; therefore, histopathological analysis followed by immunohistochemical methods is the standard for the current diagnosis.
Dominant histological features include large pleomorphic spindle and epithelioid cells with bizarre hyperchromatic nuclei, intranuclear pseudoinclusions and abundant eosinophilic cytoplasm.[1],[2] Mitoses are absent or occur rarely. Groups of large, fibrin-filled, thin-walled blood vessels are typical. The stroma of the tumor often shows hyalinization. The tumor is located subcutaneously, possibly spreading into the dermis. The margins are microscopically infiltrative. Immunohistochemically, the cells are positive for vimentin, CD99 and CD34.[1],[2]
The histopathological differential diagnosis of pleomorphic hyalinizing angiectatic tumor includes schwannoma, undifferentiated pleomorphic sarcoma and pleomorphic lipoma.[1],[2] In a schwannoma, the areas with ancient changes and hyalinized vessels may resemble pleomorphic hyalinizing angiectatic tumor, but an encapsulated schwannoma shows Verocay body formation, and the cells do not contain intracytoplasmic hemosiderin. Immunohistochemically, schwannoma cells show strong S100 protein positivity and CD34 negativity. An undifferentiated pleomorphic sarcoma is characterized by the population of highly atypical spindled or polygonal cells with marked nuclear pleomorphism and abundant atypical mitoses. Cells lack the intracytoplasmic hemosiderin and intranuclear pseudoinclusions. CD34 staining is negative or only focally positive in sarcomatous cells. In pleomorphic lipoma, strong diffuse CD34 positivity is also present as in pleomorphic hyalinizing angiectatic tumor, but the cells have a bland spindle cell morphology without mitotic figures. Typical features are the “ropey” collagen bundles and floret-like giant cells. Adipose tissue is also usually present.
The therapy of pleomorphic hyalinizing angiectatic tumor is based on a complete surgical excision of the tumor.[2],[4] Relapse of pleomorphic hyalinizing angiectatic tumor seems to occur only in cases of incomplete excision of the tumor.[1],[2] Some authors recommend a wide local excision with a 3-cm margin and an excision depth reaching deep fascia or periosteum.[2],[5] Metastases of pleomorphic hyalinizing angiectatic tumor have not yet been described.[1],[2]
In conclusion, pleomorphic hyalinizing angiectatic tumor is a rare locally aggressive soft tissue tumor which exhibits great diversity in its clinical manifestation. Histopathological examination plays a key role in the diagnosis of clinically uncertain subcutaneous lesions.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understand that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Weiss SW, Dei Tos AP. Pleomorphic hyalinizing angiectatic tumour of soft parts. In: Fletcher DM, Bridge JA, Hogendoorn PC, editors. WHO Classification of Tumours of Soft Tissue and Bone. 4th ed. Lyon: IARC Press; 2013. p. 200.
[Google Scholar]
|
| 2. |
Miettinen M. Pleomorphic hyalinizing angiectatic tumor. In: Miettinen M, editor. Modern Soft Tissue Pathology: Tumors and Non-Neoplastic Conditions. 1st ed. New York: Cambridge University Press; 2010. p. 384-7.
[Google Scholar]
|
| 3. |
Moretti VM, Brooks JS, Lackman RD. Pleomorphic hyalinizing angiectatic tumor: A clinicopathologic characterization. UPOJ 2010;20:121-4.
[Google Scholar]
|
| 4. |
Felton SJ, Ramlogan D. Spontaneous bruising overlying a subcutaneous swelling: Pleomorphic hyalinizing angiectatic tumor, a relatively new entity of intermediate malignancy. Int J Dermatol 2015;54:204-6.
[Google Scholar]
|
| 5. |
Sofos S, Tehrani H, Shaaban H. Pleomorphic hyalinizing angiectatic tumour: A tumour diagnosis of suspicion. J Med Cases 2012;3:334-6.
[Google Scholar]
|
Fulltext Views
2,977
PDF downloads
1,499





![[Figure - 1]](#fig_ijdvl_2018_84_5_619_238508_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2018_84_5_619_238508_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2018_84_5_619_238508_f3.jpg){kind=link}