Translate this page into:
Premature sebaceous hyperplasia with satisfactory response to oral isotretinoin
2 Department of Dermatology, Jining No. 1 People's Hospital, Jining, China
3 Department of Dermatology, Shandong Provincial Institute of Dermatology and Venereology, Shandong Academy of Medical Sciences, Jinan, Shandong, China
4 Department of Dermatology, Shandong Provincial Hospital for Skin Diseases, Shandong University, Jinan; Department of Dermatology, Shandong Provincial Institute of Dermatology and Venereology, Shandong Academy of Medical Sciences, Jinan, Shandong, China
Correspondence Address:
Furen Zhang
Shandong Provincial Institute of Dermatology and Venereology, 27397 Jingshi Road, Jinan, Shandong Province, 250022
China
| How to cite this article: Wang W, Qiu Y, Zhou G, Pei Z, Zhang F. Premature sebaceous hyperplasia with satisfactory response to oral isotretinoin. Indian J Dermatol Venereol Leprol 2016;82:113 |
Sir,
A 44-year-old Chinese woman presented with a cutaneous eruption affecting the face and neck since the age of 16 years [Figure - 1]a. The lesions were asymptomatic with no seasonal variation and had progressively increased over the years. She reported that her mother and sister had had similar but milder lesions since puberty [Figure - 1]c. Cutaneous examination revealed diffuse erythema with numerous soft and umbilicated, 2 to 3 mm, skin colored papules on the face, neck, and upper thorax, sparing the periorbital, perioral and perinasal areas. Some papules were confluent and formed linear patterns. Her skin was greasy. Circulating androgens (testosterone, dehydroepiandrosterone and androstenedione) and urinary 17-ketosteroids were normal. A skin biopsy showed normal epidermis and lobules of mature sebaceous glands in the dermis [Figure - 2]a. Some sebaceous ducts opened into the epidermis [Figure - 2]b. There was a mild perivascular lymphocytic infiltrate in the papillary dermis. These findings were consistent with a diagnosis of premature sebaceous hyperplasia (PSH). The patient was put on a trial of oral isotretinoin, 1 mg/kg daily for 12 weeks, resulting in significant reduction in size of the lesions and extent of facial seborrhea [Figure - 1]b. The patient reported no side-effects of isotretinoin and no relapse was observed during the 3-month follow-up period after cessation of therapy.
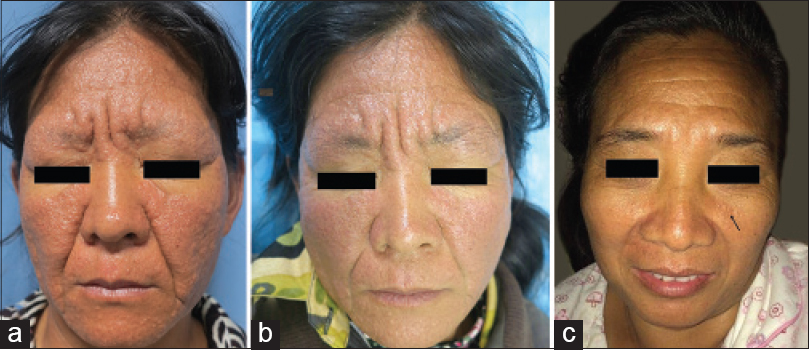 |
| Figure 1: (a) Patient before treatment. (b) Patient after 12 weeks of isotretinoin treatment. (c) Patient's sister without treatment |
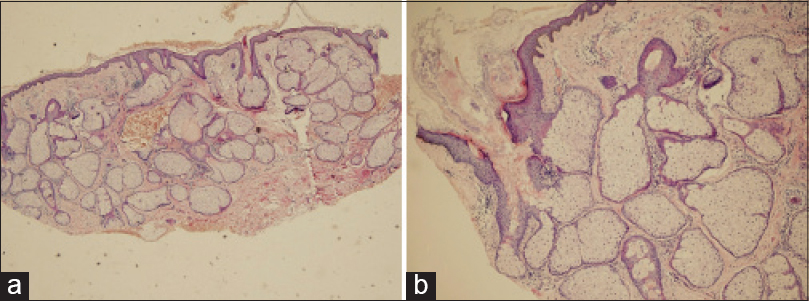 |
| Figure 2: (a) Lobules of mature sebaceous glands in the dermis (H and E, ×100). (b) Sebaceous ducts leading to the epidermis (H and E, ×400) |
Premature sebaceous hyperplasia, first reported in 1980, is a benign proliferation of sebaceous glands that appears at puberty or just afterwards and tends to become worse with age.[1] The disease has a predilection for males and is believed to have an autosomal dominant inheritance pattern. The lesions mostly occur on the face, neck and upper thorax. One of the characteristics is a lack of acneiform eruption. Histologically, there are hyperplastic and hypertrophic mature sebaceous glands, identical to those of sebaceous hyperplasia, filling the dermis.[2]
The precise etiology and pathogenesis of premature sebaceous hyperplasia remain unknown.[3] Hormonal factors were once thought to be important because most cases occur in men, but the growing incidence of the disease in women suggests there may be other factors playing a role in pathogenesis.[4] Our patient had a family history supporting genetic predisposition. However, until date, most reported cases have been sporadic. Therefore, larger case series and further research are needed to establish the etiological and pathophysiological processes of the condition.
Premature sebaceous hyperplasia may be misdiagnosed as rosacea clinically. However, histologically, the typical numerous, large sebaceous glands composed of mature sebocytes are absent in the dermis of rosacea.
Grimalt et al. reported that isotretinoin reduced the size of the sebaceous glands in 3 weeks and induced perifollicular fibrosis after 12 weeks of therapy.[5] Our patient was successfully treated with oral isotretinoin for 12 weeks. We speculate that her lack of relapse may be due to the perifollicular fibrosis secondary to isotretinoin therapy.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
| 1. |
Dupre A, Bonafé JL, Lamon R. Functional familial sebaceous hyperplasia of the face. Reverse of the Cunliffe acne-free naevus? Its inclusion among naevoid sebaceous receptor diseases. Clin Exp Dermatol 1980;5:203-7.
[Google Scholar]
|
| 2. |
Wang Q, Liu JM, Zhang YZ. Premature sebaceous hyperplasia in an adolescent boy. Pediatr Dermatol 2011;28:198-200.
[Google Scholar]
|
| 3. |
Turan H, Erdem H, Turan A, Kadioglu N, Basar F. Premature sebaceous hyperplasia with pre-pubertal onset. Int J Dermatol 2014;53:e224-6.
[Google Scholar]
|
| 4. |
Boonchai W, Leenutaphong V. Familial presenile sebaceous gland hyperplasia. J Am Acad Dermatol 1997;36:120-2.
[Google Scholar]
|
| 5. |
Grimalt R, Ferrando J, Mascaro JM. Premature familial sebaceous hyperplasia: Successful response to oral isotretinoin in three patients. J Am Acad Dermatol 1997;37:996-8.
[Google Scholar]
|
Fulltext Views
5,893
PDF downloads
2,205





![[Figure - 1]](#fig_ijdvl_2016_82_1_113_162346_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2016_82_1_113_162346_f2.jpg){kind=link}