Translate this page into:
Primary localized cutaneous nodular amyloidosis with bullous lesions
2 Zhongshan Hospital, Wuhan, China
Correspondence Address:
Changzheng Huang
Department of Dermatology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan 430022
China
| How to cite this article: Sanusi T, Li Y, Qian Y, Huang C. Primary localized cutaneous nodular amyloidosis with bullous lesions. Indian J Dermatol Venereol Leprol 2015;81:400-402 |
Sir,
A 43-year-old Chinese female presented with a 3-year history of mildly pruritic bullous skin eruptions on the upper and right lower back. Examination showed flaccid and yellowish-brown bullae surrounded by erythematous plaques on the upper back and hypopigmentation in the center and clear bullae over the right lower back. The bullae were 6 × 3.5 cm in diameter on the upper back and 1 × 1 cm in diameter on the right lower back [Figure - 1]. Mucous membranes and tongue were normal. Systemic examination revealed no abnormality.
 |
| Figure 1: (a) Bullous skin eruptions on the upper and right lower back, (b) Large bullae on the upper trunk, flaccid, and yellowish-brown color surrounded by erythematous plaque, (c) Small clear bullae on the right of the lower back |
Complete blood count, renal function, liver function and urinalysis were normal. Antinuclear antibody (ANA), extractable nuclear antigen (ENA) screen, qualitative urine porphyrin, serum protein electrophoresis and urine for Bence Jones protein were normal or negative. Roentgenogram and electrocardiogram were normal.
A skin biopsy from the edge of a bulla on the upper back showed subepidermal clefts and mass-like pink colored amorphous deposits in the papillary and reticular dermis which were positive when stained by crystal violet. Congo red staining was also positive and revealed apple-green birefringence with polarized light. There were a few plasma cells around the blood vessels [Figure - 2]. Immunohistochemistry studies showed strong positivity for λ light chain and a comparatively lesser intensity for κ light chain [Figure - 3]. Based on the clinical findings and histologic characteristics of the skin lesions, diagnosis of a primary localized cutaneous nodular amyloidosis (PLCNA) with bullous appearance was made. The lesions were removed by surgical excision.
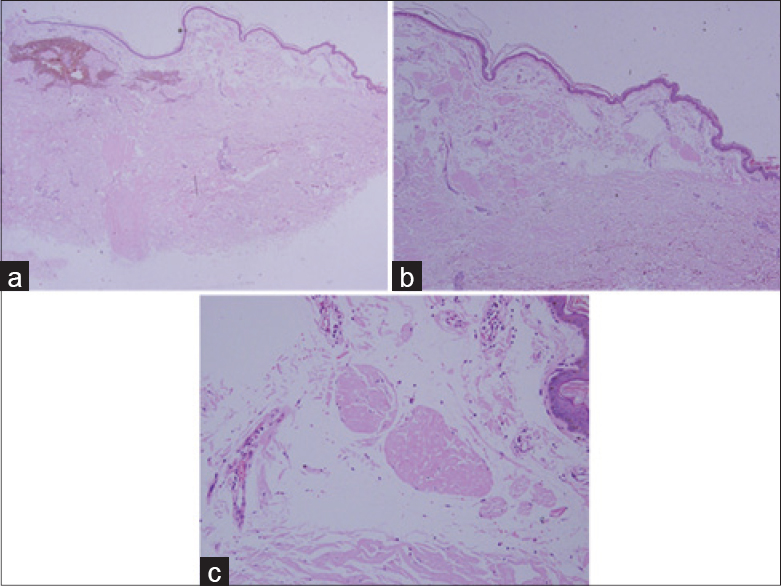 |
| Figure 2: (a and b) Subepidermal clefts and mass-like pink colored amorphous materials deposition in the papillary and reticular dermis (H and E, ×20, ×40), (c) Plasma cells infiltration around the blood vessels (H and E, ×200) |
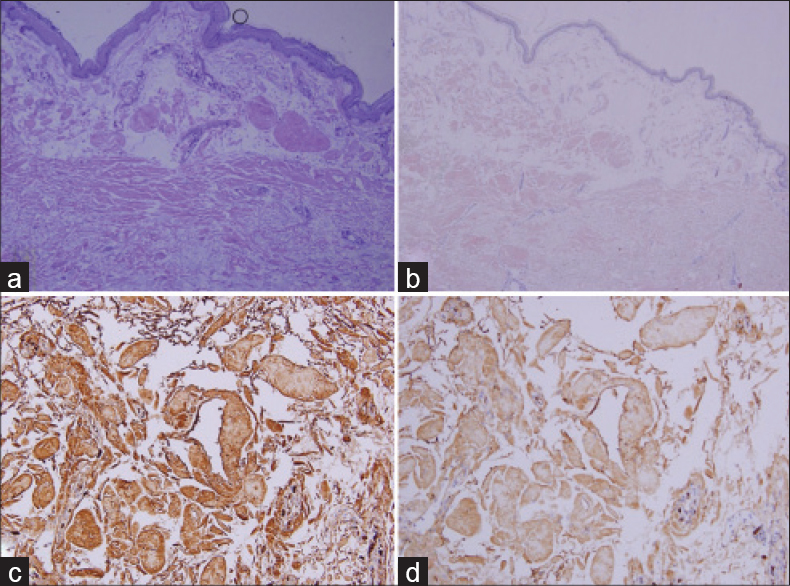 |
| Figure 3: (a) Subepidermal cleft and amyloid deposition in the entire dermis was positive with violet staining (×100) and (b) Congo red staining (×40), also positive for apple-green birefringence with polarized light (not shown). (c) Immunohistochemistry staining showed strong positivity for λ light chain (×200) and (d) less intensity for κ light chain (×200) |
Primary localized cutaneous nodular amyloidosis is a rare variant of cutaneous amyloidosis. Approximately 100 cases of nodular cutaneous amyloidosis have been reported in the medical literature. [1] Cutaneous nodular amyloidosis is composed of light-chain immunoglobulins (AL amyloid) derived from a monoclonal expansion of plasma cells. The amyloid infiltrates the entire dermis from the papillary dermis to the subcutis. The amyloid deposits may also be seen in the vessels and nerve sheath. The condition commonly occurs on the legs, feet, trunk, face and genitalia. It presents typically with single or multiple waxy yellow-red nodules. [2] However, the lesions may be indistinguishable from cutaneous lesions of primary systemic amyloidosis. Immunohistochemical analysis of the dermal deposits of amyloid has revealed that the light chains may be λ or κ, or that both may be present. [3]
Bullous lesions of cutaneous amyloidosis are commonly associated with systemic amyloidosis with multiorgan involvement, including primary systemic amyloidosis and myeloma-associated amyloidosis. However, several patients of localized bullous cutaneous amyloidosis without systemic involvement have been described. [4] The bullae can be either intradermal or subepidermal, often induced by trauma or friction which are described as tense painful blisters that are frequently hemorrhagic. [5]
The mechanism of blister formation in cases of cutaneous amyloidosis remains to be described. Ochiai et al.[4] suggested that the amyloid globules might be engulfed through the process of transepidermal elimination initiated by trauma or rubbing which are induced by persistent pruritus that acts as the local precipitating factor for blister formation.
The treatment of primary localized cutaneous nodular amyloidosis includes surgical excision, cryotherapy, electrodesiccation and curettage, intralesional steroid injection and treatment with the CO 2 laser, each with different results. Nevertheless, the lesions are difficult to treat and often recur after treatment. The progression of primary localized cutaneous nodular amyloidosis to systemic amyloidosis has been reported in some case series at the rate of 7-50%. [3] Electron microscopy has shown that the deposits of amyloid, either primary or secondary type, consist of accumulation of rigid non-branching fibrils which are responsible for the Congo Red birefringence seen on polarized light microscopy. [2],[5] Systemic evaluation and long-term follow-up is needed to monitor the progression to systemic amyloidosis. We were able to find only one previous report of this presentation. [6]
| 1. |
Santos-Juanes J, Galache C, Curto JR, Astudillo A, Sanchez del Rio J. Nodular primary cutaneous amyloidosis. J Eur Acad Dermatol Venereol 2004;18:224-6.
[Google Scholar]
|
| 2. |
Fernandez-Flores A. Cutaneous amyloidosis: A concept review. Am J Dermatopathol 2012;34:1-14.
[Google Scholar]
|
| 3. |
Woollons A, Black MM. Nodular localized primary cutaneous amyloidosis: A long-term follow-up study. Br J Dermatol 2001;145:105-9.
[Google Scholar]
|
| 4. |
Ochiai T, Morishima T, Hao T, Takayama A. Bullous amyloidosis: The mechanism of blister formation revealed by electron microscopy. J Cutan Pathol 2001;28:407-11.
[Google Scholar]
|
| 5. |
Lachmann HJ, Hawkins PN. Amyloidosis of the Skin. In: Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, Wolff K, editors. Fitzpatrick′s dermatology in general medicine. 8 th ed. New York: McGraw-Hill; 2012. p. 1574-83.
[Google Scholar]
|
| 6. |
LaChance A, Phelps A, Finch J, Lu J, Elaba Z, Rezuke W, et al. Nodular cutaneous amyloidosis: A bullous variant. Clin Exp Dermatol 2014;39:344-7.
[Google Scholar]
|
Fulltext Views
3,547
PDF downloads
1,606





![[Figure - 1]](#fig_ijdvl_2015_81_4_400_157459_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2015_81_4_400_157459_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2015_81_4_400_157459_f3.jpg){kind=link}