Translate this page into:
Progressive Nagashima-type palmoplantar keratosis in a Chinese patient with recurrent c.796C>T mutation in SERPINB7
Correspondence Address:
Xian-Biao Zou
Department of Dermatology, First Affiliated Hospital of PLA General Hospital, No. 51 Fucheng Road, Beijing 100048
People's Republic of China
| How to cite this article: Qiu M, Zou XB. Progressive Nagashima-type palmoplantar keratosis in a Chinese patient with recurrent c.796C>T mutation in SERPINB7. Indian J Dermatol Venereol Leprol 2017;83:136 |
Sir,
Nagashima-type palmoplantar keratosis (OMIM 615598) is a mild form of diffuse, transgradient palmoplantar keratoderma which was first described in Japan.[1] Clinically, it is characterized by diffuse hyperkeratosis with erythema extending to the dorsum of hands and feet, wrists, ankles and Achilles tendon. Recently, it has been associated with loss-of-function mutations in SERPINB7.[2] Depletion of SERPINB7, a specific serine protease, may lead to excessive degradation of epidermal proteins resulting in enhanced water permeation of stratum corneum and consequent hyperkeratosis.[2] Herein we report a severe, progressive case of Nagashima-type palmoplantar keratosis with a recurrent homozygous mutation c.796C>T in SERPINB7.
The patient was a 28-year-old woman of Chinese Han ethnicity, born of a non-consanguineous marriage. She was apparently normal at birth. At 7 months of age, she was noted to have scaly erythema on the palms and soles. Thereafter, she developed diffuse reddish hyperkeratosis with scaling that gradually extended to the dorsum of her hands and feet, wrists and ankles. Notably, the condition continued to progress after puberty to involve her distal forearms, elbows, shins, knees, lower thighs and perianal area with intense pruritus [Figure - 1]a,[Figure - 1]b,[Figure - 1]c. Leukokeratosis and fissures were found on her tongue but the rest of the buccal mucosa was spared [Figure - 1]d. She also reported mild palmoplantar hyperhidrosis and had suffered repeated episodes of tinea pedis. Whitish, spongy change was observed on her palms and soles after contact with water for about 2 minutes. Her mother, too was noted to have mild thickening and redness of the palmoplantar skin extending to the marginal areas. The mother had also noticed a whitish spongy change after water exposure for 6 years, which did not progress [Figure - 1]e and [Figure - 1]f. The patient and her mother were otherwise healthy and had no significant systemic illnesses other than a history of asthma and allergic rhinitis in the patient. No other family members were reported to suffer from similar symptoms.
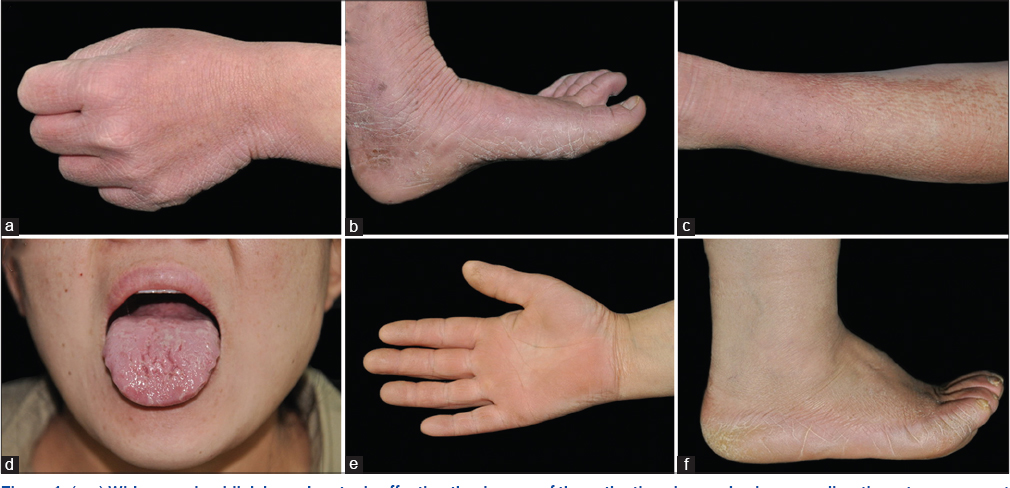 |
| Figure 1: (a-c) Widespread reddish hyperkeratosis affecting the dorsum of the patient's palms and soles, as well as the extensor aspect of her shin. (d) Leukokeratosis and fissures on the patient's tongue. (e and f) Mild palmoplantar keratoderma extending to the margins, in the patient's mother |
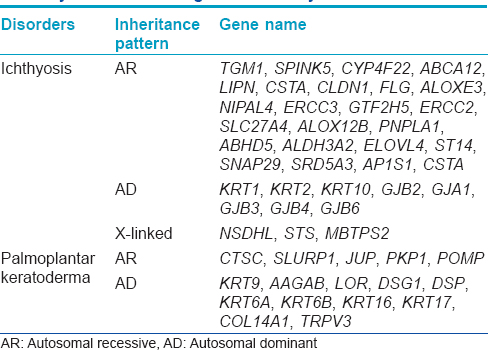
Genomic DNA was extracted from the peripheral white blood cells for further studies after getting approval from the institutional ethics committee and informed consent from the participants. We performed the Sanger sequencing method in all coding and flanking sequences of SERPINB7 gene in the family and detected a homozygous mutation c.796C>T (p. Arg266*) in SERPINB7 in the patient, which was heterozygous in her mother [Figure - 2] and her unaffected brother (her father was deceased, thus no DNA samples were available). In addition, mutations in 51 other genes known to be associated with inherited ichthyosis or palmoplantar keratoderma were excluded by next-generation target sequencing [Table - 1].
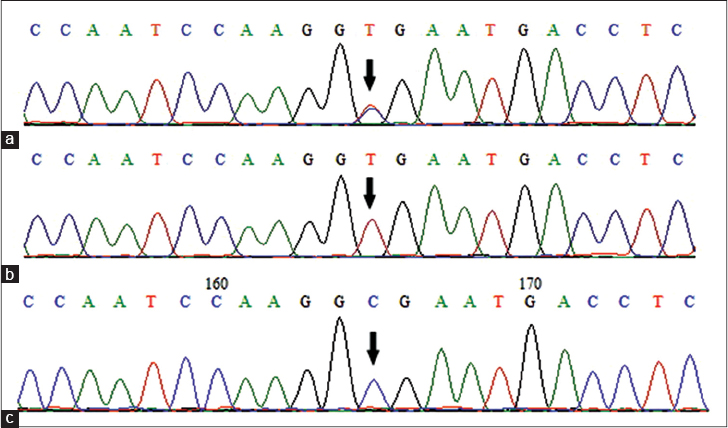 |
| Figure 2: Genomic DNA sequencing (a) of the patient's mother, (b) the patient and (c) a normal individual |
Kubo et al. recently identified SERPINB7 as the causative gene of Nagashima-type palmoplantar keratosis. They detected three different loss-of-function mutations in SERPINB7 in 13 unrelated Japanese individuals with this condition.[2] Of note, all the patients in their study harbored a nonsense mutation c.796C>T in SERPINB7, either homozygous or compound heterozygous. Later, Yin et al. reported seven unrelated Chinese patients with this condition and identified the recurrent c.796C>T mutation in SERPINB7 in six patients.[3] Interestingly, according to the 1000 Genomes Project, c.796C>T (rs142859678) is prevalent in the normal Japanese and Chinese population with frequencies of 1.12% and 1.52%, respectively. It is putatively the most common form of palmoplantar keratoderma in Japan and China and therefore, the mutation c. 796C>T was suggested to be screened preferentially in patients suspected to have this condition.[3]
To date, there are eight different mutations in SERPINB7 reported, including four predicted to affect splicing sites (c.455-1G>A, c.455G>T, c.336 + 2T>G, and c.218_219delinsTAAACTTTACCT), two frameshift mutations (c.522-523insT and c.650_653del), one nonsense mutation (c.796C>T) and one missense mutation (c.830C>T).[2],[3],[4],[5] No obvious genotype-phenotype correlation has been determined and no remarkable difference in clinical severity between patients harboring different mutations have been identified. Interestingly, skin lesions continued to progress even after puberty in our patient, in contrast to the typical non-progressive course after childhood in most patients. She also had much more widespread lesions involving the shins, lower thighs, distal forearms and perianal areas, as well as leukokeratosis and fissuring of her tongue which were not reported in patients with Nagashima-type palmoplantar keratosis previously. Since no pathogenic mutations in other known causative genes for ichthyosis and palmoplantar keratoderma were detected in the proband, we reasoned that homozygous mutation c.796C>T in SERPINB7 probably contributed greatly, if not fully, to this unusual phenotype. Furthermore, the mother, who is a heterozygous carrier of c.796C>T, showed mild non-progressive palmoplantar keratoderma since childhood. Since pseudodominant-inheritance pattern has been reported in a family with this condition, we sequenced all the coding and flanking sequences of SERPINB7 in the mother but no additional mutations or variants were detected.[4] As the patient's brother, who was a heterozygous carrier for the mutation, was not affected, we inferred that added genetic deficiencies, for example, loss-of-function mutations in other serpin genes that are expressed in skin such as SERPINB3, SERPINB4 or SERPINB8, may play an important role in the phenotypic expression and clinical severity of the disease in the family. Further studies are required to verify this hypothesis.
Acknowledgment
We are grateful to the patient and her family members for their participation in this study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Kabashima K, Sakabe J, Yamada Y, Tokura Y. “Nagashima-type” keratosis as a novel entity in the palmoplantar keratoderma category. Arch Dermatol 2008;144:375-9.
[Google Scholar]
|
| 2. |
Kubo A, Shiohama A, Sasaki T, Nakabayashi K, Kawasaki H, Atsugi T, et al. Mutations in SERPINB7, encoding a member of the serine protease inhibitor superfamily, cause Nagashima-type palmoplantar keratosis. Am J Hum Genet 2013;93:945-56.
[Google Scholar]
|
| 3. |
Yin J, Xu G, Wang H, Zhao J, Duo L, Cao X, et al. New and recurrent SERPINB7 mutations in seven Chinese patients with Nagashima-type palmoplantar keratosis. J Invest Dermatol 2014;134:2269-72.
[Google Scholar]
|
| 4. |
Mizuno O, Nomura T, Suzuki S, Takeda M, Ohguchi Y, Fujita Y, et al. Highly prevalent SERPINB7 founder mutation causes pseudodominant inheritance pattern in Nagashima-type palmoplantar keratosis. Br J Dermatol 2014;171:847-53.
[Google Scholar]
|
| 5. |
Shiohama A, Sasaki T, Sato S, Sakabe JI, Ito T, Isoda H, et al. Identification and characterization of a recessive missense mutation p.P277L in SERPINB7 in Nagashima-type palmoplantar keratosis. J Invest Dermatol 2015;136:325-8.
[Google Scholar]
|
Fulltext Views
3,097
PDF downloads
2,988





![[Figure - 1]](#fig_ijdvl_2017_83_1_136_187093_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2017_83_1_136_187093_f2.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2017_83_1_136_187093_t3.jpg){kind=link}