Translate this page into:
Pustular rheumatoid neutrophilic dermatitis with Koebner phenomenon
2 Department of Dermatology, Shandong Provincial Institute of Dermatology and Venereology, Shandong Academy of Medical Sciences, Jinan, Shandong, China
3 Department of Dermatology, Qilu Hospital of Shandong University, Jinan, Shandong, China
4 Department of Dermatology, Shandong Provincial Hospital for Skin Diseases, Shandong University; Department of Dermatology, Shandong Provincial Institute of Dermatology and Venereology, Shandong Academy of Medical Sciences, Jinan, Shandong, China
Correspondence Address:
Keyu Wang
Department of Dermatology, Qilu Hospital of Shandong University, 107 Wenhua Xi Road, Jinan, Shandong 250012
China
| How to cite this article: Zhang K, Zhou G, Yu C, Wang K, Zhang F. Pustular rheumatoid neutrophilic dermatitis with Koebner phenomenon. Indian J Dermatol Venereol Leprol 2016;82:569-571 |
Sir,
Rheumatoid neutrophilic dermatitis is a rare cutaneous disorder associated with rheumatoid arthritis (RA).[1] It is observed predominantly in middle-aged women with severe rheumatoid arthritis and has been associated with relatively high titers of rheumatoid factor (RF).[2] It commonly manifests as symmetric erythematous plaques, papules, nodules or palpable purpura over the trunk, shoulders, neck or extensor aspects of extremities.[3] We report here a case of pustular rheumatoid neutrophilic dermatitis with Koebner phenomenon; we found only one previous report of this disease with the phenomenon.[4]
A 56-year-old Chinese female with a 16-year history of rheumatoid arthritis was referred to our hospital for skin lesions for 5 months. Pruritic skin lesions had appeared on her legs 3 months before admission and had gradually increased. She had been taking leflunomide, 10 mg daily, orally and Tripterygium wilfordii (20 mg tid) for many years. Administration of antibacterial drugs had no effect on the course of skin lesions. Dermatological examination revealed numerous erythematous plaques, papules and tense pustules, symmetrically distributed over the lumbosacral area, buttocks, dorsum of the hands and extensor surfaces of the lower legs. The pustules were about 1-10 mm in diameter, some of which surrounded the erythematous areas with a semi-ring-like appearance [Figure - 1]a and [Figure - 1]b. In particular, two linear areas of erythema were noted on the right thigh which contained multiple papules and pustules suggestive of Koebner phenomenon; [Figure - 2].
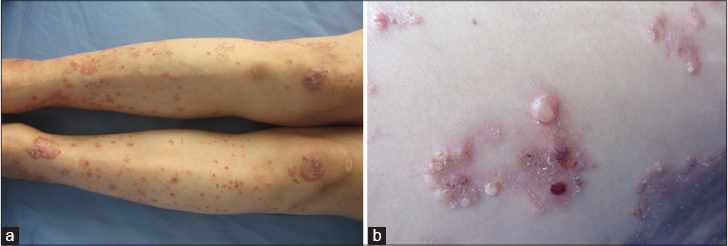 |
| Figure 1: (a) Erythematous plaques, papules and pustules were symmetrically distributed on the extensor surfaces of the lower legs. (b) Pustules having a semi-ring-like appearance surrounded the erythema |
 |
| Figure 2: Linear erythema on the right thigh, with multiple overlying papules and pustules (Koebner phenomenon) |
A skin biopsy taken from one of the erythematous areas on the right thigh showed a subepidermal pustule with neutrophils and nuclear dust scattered around the vessels and between collagen fibers in the upper dermis and mid-dermis, but without vasculitis [Figure - 3]a and [Figure - 3]b. Immunofluorescence was negative. Laboratory examination revealed a normal leucocyte count, an erythrocyte sedimentation rate of 23 mm/h and a rheumatoid factor (RF) titre of 515.2 IU/mL (reference range: 0-10 IU/mL). An extractable nuclear antigen antibody test revealed strongly positive ribonucleoprotein (RNP)/Sm, anti-Ro-52 and antinuclear antibodies (ANA) and negative SSA, SSB, Sm, double stranded-DNA and ANCA antibodies. Serology for human immunodeficiency virus (HIV), hepatitis B virus, and hepatitis C virus (HCV) were all negative. Erosions were detected on radiographs of the left knee joint and the chest X-ray revealed bronchitis. Based on her history, clinical manifestations, histological and other laboratory findings, a diagnosis of rheumatoid neutrophilic dermatitis was established.
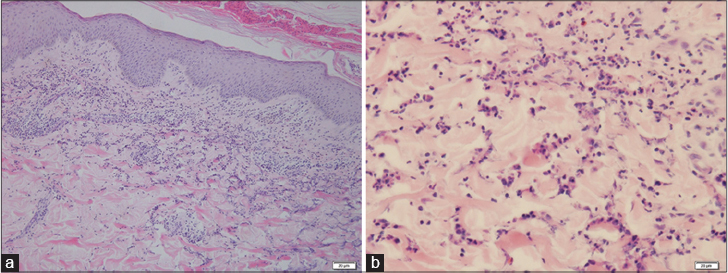 |
| Figure 3: (a) A subepidermal pustule. Dense inflammatory cells were found in the upper dermis and mid-dermis (H and E, ×100). (b) Neutrophils and nuclear dust were scattered around the blood vessels and amid the collagen, without vasculitis (H and E, ×400) |
Rheumatoid neutrophilic dermatitis must be differentiated from other neutrophilic dermatoses such as Sweet's syndrome, pyoderma gangrenosum, erythema elevatum diutinum, Behcet's syndrome and bowel bypass syndrome.[3] Among these diseases, differentiating rheumatoid neutrophilic dermatitis from Sweet's syndrome is the most difficult due to similar clinical and histopathological presentations. In our case, the lesions were located symmetrically and scattered throughout the trunk and limbs in contrast to Sweet's syndrome. Since our case was clinically similar to pustular psoriasis and psoriatic arthritis, these conditions should be considered, as well. However, histologically, the infiltrate is deeper than in psoriasis. Moreover, our patient had no personal or family history of psoriasis and had high positive titers of RF, RNP and ANA, all of which suggested the dermatosis to be rheumatoid neutrophilic dermatitis.
From a clinical point of view, our patient had two unusual characteristics: first, widely distributed pustules are rarely reported in rheumatoid neutrophilic dermatitis; second, the most prominent manifestation was the Koebner phenomenon. Koebner phenomenon can be seen in various inflammatory, autoimmune, viral, fibrotic, rheumatic and even tumoral disorders apart from the well known occurrence in psoriasis, lichen planus and vitiligo. Furthermore, this phenomenon is not restricted to the skin; in some rheumatic diseases, it also sometimes occurs in internal organs.[4],[5] Rheumatoid arthritis and various skin diseases that occur in association with it such as rheumatoid nodule, rheumatoid neutrophilic dermatitis, palisaded neutrophilic granulomatous dermatitis, often present with cutaneous manifestations with this phenomenon.[4] The phenomenon may follow mechanical or thermal trauma, dermatoses, allergic or irritant reactions and therapy. Nonsteroidal anti-inflammatory and some other drugs may exacerbate psoriasis and induce koebnerization.[6] Koebner phenomenon appeared in our case after mechanical trauma. Because the patient had taken leflunomide for many years and the skin lesions appeared only 3 months before admission, we did not think leflunomide to be the cause of the rash. The pathogenesis of the Koebner phenomenon is still unclear. However, the second-step theory proposed by Ueki et al. to elaborate the phenomenon may help us understand it.[5]
Boyd and Neldner have classified all reported cases of the Koebner phenomenon into four types.[6] Although it is not clear which type it was in our case, as this needs additional studies and reports, the presence of Koebner's phenomenon does signify disease activity. It may also guide us in avoiding physical and chemical irritants and other trauma when treating underlying or concurrent rheumatoid neutrophilic dermatitis in order to better manage the disease. The patient was treated with azithromycin, 500 mg once daily, parenterally, prednisone, 10 mg once daily, orally, T. wilfordii, 20 mg 3 times a day orally and colchicine, 500 µg twice daily, orally. All the pustules gradually vanished and the erythema darkened after 1 week of treatment. During the 5 months follow-up period, the patient's arthritis came under control and no recurrence of the skin lesions was observed after reduction of the prednisone. Currently, disease control is being maintained with prednisone (5 mg once daily), T. wilfordii (20 mg tid) and colchicine (500 µg twice daily).
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Ergun T, Inanc N, Tuney D, Kotiloglu EK, Seckin D, Tetik C, et al. Skin manifestations of rheumatoid arthritis: A study of 215 Turkish patients. Int J Dermatol 2008;47:894-902.
[Google Scholar]
|
| 2. |
Brown TS, Fearneyhough PK, Burruss JB, Callen JP. Rheumatoid neutrophilic dermatitis in a woman with seronegative rheumatoid arthritis. J Am Acad Dermatol 2001;45:596-600.
[Google Scholar]
|
| 3. |
Lazarov A, Mor A, Cordoba M, Mekori YA. Rheumatoid neutrophilic dermatitis: An initial dermatological manifestation of seronegative rheumatoid arthritis. J Eur Acad Dermatol Venereol 2002;16:74-6.
[Google Scholar]
|
| 4. |
Yamamoto T, Ueki H. Koebner phenomenon in rheumatoid arthritis. J Genet Syndr Gene Ther 2013;4:173.
[Google Scholar]
|
| 5. |
Ueki H. Koebner phenomenon in lupus erythematosus with special consideration of clinical findings. Autoimmun Rev 2005;4:219-23.
[Google Scholar]
|
| 6. |
Boyd AS, Neldner KH. The isomorphic response of Koebner. Int J Dermatol 1990;29:401-10.
[Google Scholar]
|
Fulltext Views
3,844
PDF downloads
1,023





![[Figure - 1]](#fig_ijdvl_2016_82_5_569_183637_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2016_82_5_569_183637_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2016_82_5_569_183637_f3.jpg){kind=link}