Translate this page into:
Reactive eccrine syringofibroadenoma on a leprous foot
2 Department of Pathology, Medical College Kolkata, Kolkata, West Bengal, India
Correspondence Address:
Debabrata Bandyopadhyay
Department of Dermatology, Venereology and Leprosy, Medical College Kolkata, 88, College Street, Kolkata - 700 073, West Bengal
India
| How to cite this article: Bandyopadhyay D, Chattopadhyay S, Saha S. Reactive eccrine syringofibroadenoma on a leprous foot. Indian J Dermatol Venereol Leprol 2015;81:64-66 |
Eccrine syringofibroadenoma (ESFA) is a rare benign neoplasm with eccrine ductal differentiation. The condition usually presents as a solitary, often large, hyperkeratotic plaque or nodule with a predilection for the extremities but may have several clinical variants and associations. The histopathology of the condition is distinctive [1] and shows thin anastomosing epithelial cords and strands forming a lattice and connected to the undersurface of the epidermis. Ducts are present within the tumor, which is embedded in a rich fibrovascular stroma. Five subtypes are recognized: (1) solitary, (2) multiple with hidrotic ectodermal dysplasia, (3) multiple, without associated cutaneous findings, (4) nonfamilial unilateral, linear (or nevoid), and (5) reactive, associated with inflammatory or neoplastic dermatoses. [2] We present here a case of the reactive type in association with leprosy. We were able to find only two previous reports of leprosy-associated reactive eccrine syringofibroadenoma. [3],[4]
A 52-year-old man was referred to us for the evaluation of an ulcer over his left sole for the last two years. The patient had a history of borderline tuberculoid leprosy involving his left lower limb and trunk, and he was released from treatment three years previously after completion of multidrug therapy. His foot had remained insensitive since then and he developed thickening of the sole with an ulcer for which he was treated intermittently with various medications. His family history and past medical history were unremarkable. Examination revealed thick keratoderma involving the posterior two-third of the sole of the left foot and a deep-seated ulcer with a clean floor on the lateral side of the sole within the keratotic area [Figure - 1]. The foot and lower leg was insensitive to touch and pain. There was no nerve thickening or regional lymphadenopathy. The remainder of the mucocutaneous and systemic examination was non-contributory. Routine laboratory examinations and serum biochemistry panel were normal. No abnormality was detected on X-ray of the foot. Culture from the ulcer was sterile and slit skin smear from the lesions was negative. Biopsy from the ulcer showed features of chronic non-specific inflammation, while the specimen from the hyperkeratotic area showed hyperkeratosis and thin anastomotic strands of epithelial cells emerging from the undersurface of the epidermis [Figure - 2]. The strands were embedded within a fibrovascular stroma and contained eccrine lumen-like structures at certain places [Figure - 3]. Based on the history, clinical findings and characteristic histopathology, a final diagnosis of trophic ulcer in a treated case of leprosy with reactive syringofibroadenoma was made and the patient was advised conservative management with appropriate foot care, topical emollients and keratolytics, and regular follow-up. Clinical review after six months of presentation revealed signs of healing of the ulcer and mild improvement of hyperkeratosis.
 |
| Figure 1: Keratoderma and ulcer on the left sole |
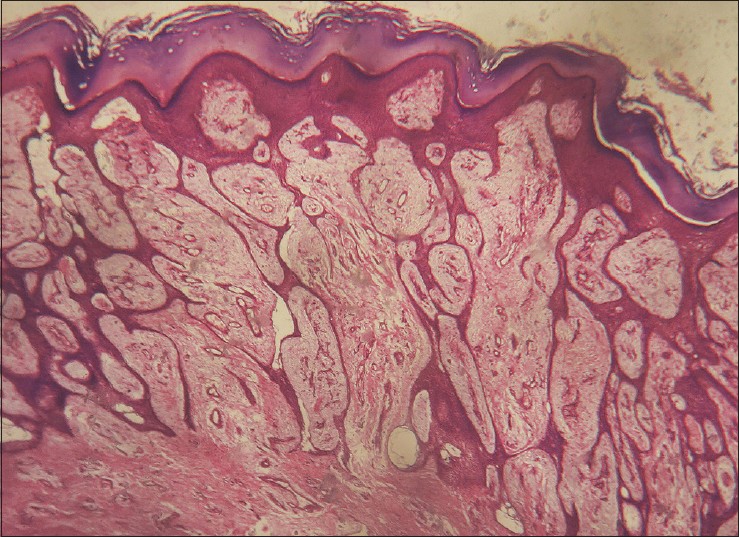 |
| Figure 2: Anastomosing thin cords of epithelial cells containing luminal structures within a fibrovascular stroma. (H and E stain; original magnification ×l00) |
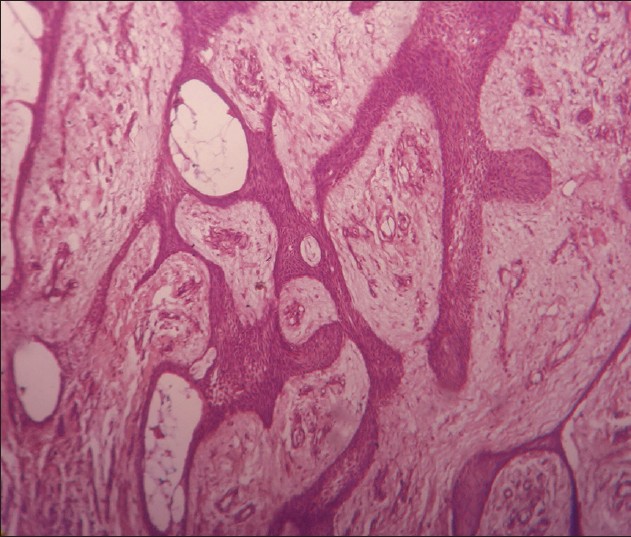 |
| Figure 3: Ductal lumina are seen within the anastomosing epithelial cords. (H and E stain; original magnification ×200) |
The phenomenon of occurrence of eccrine syringofibroadenoma next to inflammatory dermatoses and tumors, often in an acral location, has been called reactive eccrine syringofibroadenoma. For the diffuse reactive form, the terms ′acrosyringeal adenomatosis and ′eccrine syringofibroadenomatosis′ have been suggested as appropriate designations. [1] Fewer than 25 cases of reactive eccrine syringofibroadenoma appear to have been reported in the literature. This reactive change has been previously reported to occur in association with palmoplantar erosive lichen planus, bullous pemphigoid, burn scar, ileostomy stoma, venous stasis, nevus sebaceous, and chronic diabetic foot ulcer. [1],[2] Reactive eccrine syringofibroadenoma associated with lepromatous leprosy has been documented previously, the patient having multiple verrucous plaques over the foot. [3] Partial spontaneous regression of such a lesion has been documented. [4] The condition has also occurred on diffuse plantar hyperkeratosis, as in our case. [5] The pathogenesis of reactive eccrine syringofibroadenoma is uncertain, and it has been suggested that it may result from repeated eccrine duct trauma resulting in eccrine duct remodeling and repair. [6] Such traumatic events are more likely to result from the insensitivity of the feet caused by leprosy. The possibility of a neuroeccrine interaction, with sympathetic neuropathy in leprosy as a contributing factor in the pathogenesis has also been considered. [3] Moreover, most cases of the reactive type occurred on the lower legs or feet in association with conditions of impaired blood circulation. [7]
Eccrine syringofibroadenoma generally pursues a benign course. However, excision of the lesion is recommended for solitary circumscribed lesions since malignant transformation has been reported. Since the risk is very low, close observation and follow-up is an alternative, especially when complete excision is impractical due to involvement of larger areas as in our case. [2]
| 1. |
Weedon D. Weedon's Skin Pathology. 3 rd ed. London: Churchill Livingstone, Elsevier, 2010.
rd ed. London: Churchill Livingstone, Elsevier, 2010.'>[Google Scholar]
|
| 2. |
Cho E, Lee JD, Cho SH. A case of reactive eccrine syringofibroadenoma. Ann Dermatol 2011;23:70-2.
[Google Scholar]
|
| 3. |
Tey HL, Chong WS, Wong SN. Leprosy-associated eccrine syringofibroadenoma of Mascaro. Clin Exp Dermatol 2007; 32:533-5.
[Google Scholar]
|
| 4. |
Tey HL. Characterizing the nature of eccrine syringofibroadenoma: Illustration with a case showing spontaneous involution. Clin Exp Dermatol 2009;34:e66-8.
[Google Scholar]
|
| 5. |
Kawaguchi M, Takeda H, Mitsuhashi Y, Kondo S. Eccrine syringofibroadenoma with diffuse plantar hyperkeratosis. Br J Dermatol 2003;149:885-6.
[Google Scholar]
|
| 6. |
Mattoch IW, Pham N, Robbins JB, Bogomilsky J, Tandon M, Kohler S. Reactive eccrine syringofibroadenoma arising in peristomal skin: An unusual presentation of a rare lesion. J Am Acad Dermatol 2008;58:691-6.
[Google Scholar]
|
| 7. |
Utani A, Yabunami H, Kakuta T, Endo H, Shinkai H. Reactive eccrine syringofibroadenoma: An association with chronic foot ulcer in a patient with diabetes mellitus. J Am Acad Dermatol 1999;41:650-1.
[Google Scholar]
|
Fulltext Views
2,924
PDF downloads
3,210





![[Figure - 1]](#fig_ijdvl_2015_81_1_64_148578_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2015_81_1_64_148578_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2015_81_1_64_148578_f3.jpg){kind=link}