Translate this page into:
Recurrent Spitz nevus with multiple satellite lesions on perineum
Correspondence Address:
H Sang
Professor, Jinling Hosp, Dept Dermatology, Nanjing Univ, Sch Med, Nanjing 210002, Peoples R China
China
| How to cite this article: Chen J, Kong Q T, Zhang M, Sang H. Recurrent Spitz nevus with multiple satellite lesions on perineum. Indian J Dermatol Venereol Leprol 2015;81:96 |
Sir,
Spitz nevus (SN) is a benign melanocytic lesion that usually does not recur after partial or full excision. We report a case of a seven-year-old boy with a solitary Spitz nevus on perineum which recurred as multiple satellite lesions one month after the original lesion was completely removed.
A seven-year-old Chinese boy originally presented to his local hospital with a solitary purple nodule, approximately the size of 0.5 cm × 0.6 cm on his perineum, which was completely excised. Histopathological examination showed it to be a typical Spitz nevus; nevus cells were not present in the histopathology margins. One month after the surgery, multiple satellite lesions appeared close to the primary operative site and gradually increased in size, becoming slightly elevated. On physical examination, there was a solid purple nodule approximately 0.4 × 0.5 cm, with two nodules, arranged as satellite lesions [Figure - 1]. Family history of skin cancer was denied. An excision of the main nodule and the nearest satellite lesion was performed again while the second satellite nodule was not excised. Histopathologic examination of the two excised lesions showed different features: the main nodule revealed a proliferation of spindle cell melanocytes arranged as nests, distributed symmetrically at the dermoepidermal junction, and as fascicles in the papillary and reticular dermis while the satellite lesion showed nevus cells exclusively in the dermis. There was no evidence of cytologic atypia in either lesion [Figure - 2]. Immunohistochemical staining showed that neoplastic cells were strongly positive for S100 [Figure - 3] and Mel-A protein [Figure - 4] but negative for SMA and HMB45 protein, and the Ki67 labelling index was less than 5%. In view of the clinical, histopathologic and immunohistochemical features, a diagnosis of Spitz nevus was made. Follow-up examination showed that the two excised lesions did not recur, while the satellite nodule that was left un-excised has shown no change so far.
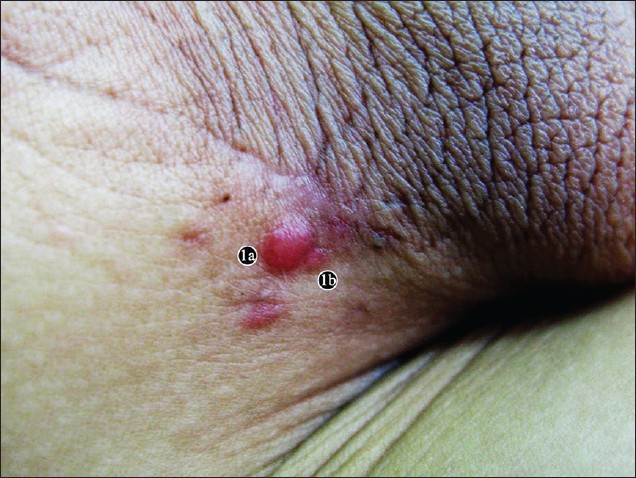 |
| Figure 1: On the right side of the perineum, a solid purple nodule about 0.4 cm × 0.5 cm (a), with two nodules approximately 0.2 cm × 0.1 cm (b), arranged as satellite lesions |
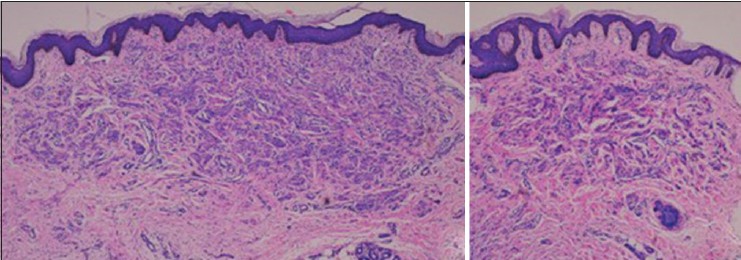 |
| Figure 2: (a) Main nodule: A proliferation of spindle cells arranged as nests, distributed at the dermoepidermal junction and in fascicles in the papillary and reticular dermis. (b) Satellite nodule: Spindle cells are seen in the reticular dermis. (hematoxylin counterstain, original magnification, ×40) |
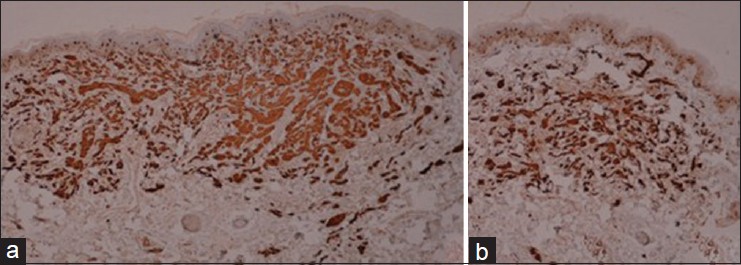 |
| Figure 3: (a and b) The spindle cells are strongly positive for S-100 protein staining (original magnification, ×40) |
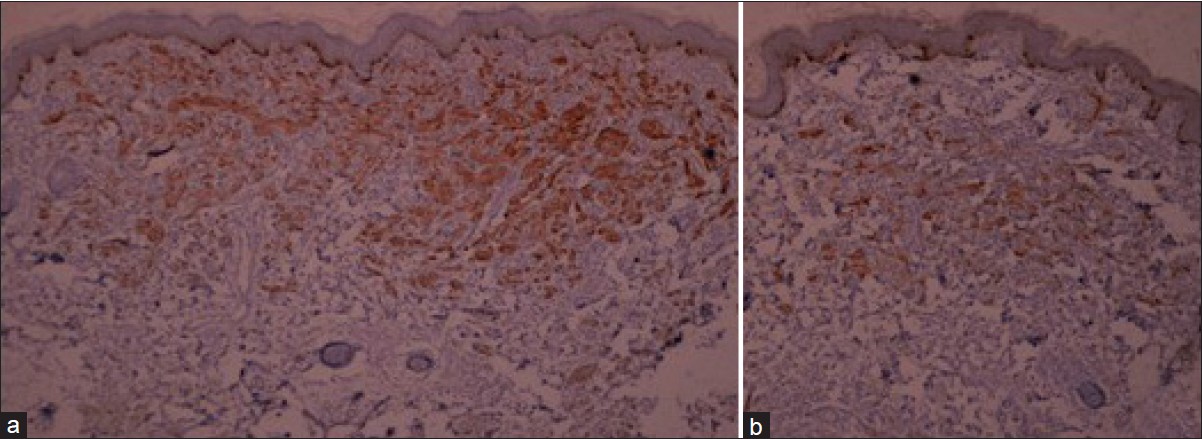 |
| Figure 4: (a and b) The spindle cells are positive for Mel-A protein (original magnification, ×40) |
Spitz nevus is generally considered a childhood lesion but recent reports show that a significant number (37-60%) are diagnosed in patients older than 20 years. [1]
The nevus occurs predominantly on the head. However, a significant number may occur on other locations. Berlingeri-Ramos et al.[1] recently reported that a predominant location of Spitz nevus is the lower extremities, followed by the upper extremities. The least common among the involved anatomic locations were the head, neck, and trunk. Even though the occurrence of Spitz nevus on the perineum is rare, it has also been reported at other unusual locations such as fingernail, oral cavity, and tongue.
Spitz nevus commonly appears as a solitary, dome-shaped, firm, red, or brown nodule. while multiple nevi are extremely rare. [2] Multiple Spitz nevi can be classified into four categories: Disseminated, grouped and arising on normal skin, grouped and arising on a hypopigmented macule, and grouped and arising on a congenital pigmented macule. Our report shows a special type, satellite pattern with a solid purple nodule along with other two nodules. We were able to find only one previous report of this pattern. In 2005, Song et al. [3] reported a 19-year-old Korean woman with multiple satellite lesions on her abdomen. The reason for this phenomenon is still unknown and it may clinically mimic melanoma. Zaenglein et al. [4] reported an infant with a congenital Spitz nevus on the scalp exhibiting clinical features of melanoma, including variegation and regression of pigmentation and a rapidly changing appearance. Recurrence after excision, as in our case, is another feature that may mimic melanoma. In our case, the recurrence appears to have been induced by excision. Carmelo Urso [5] reported the histologic features in 6 cases of Spitz tumors, 2 of which metastasized to regional lymph nodes and suggested that the Spitz tumor may be malignant in some cases.
Typical Spitz nevi can be junctional, compound, or intradermal with spindle cell melanocytes arranged in nests. In our patient, the larger, central recurrent lesion showed features of a compound nevus while the smaller lesion showed an intradermal nevus. ′′Maturation′′ of cells with increasing depth; lack of mitoses and single-cell upward spread; and negative/low level staining with immunohistochemical stains, such as HMB-45 and Ki-67, help to identify benign lesions. [6]
Since the presentation of recurrent Spitz nevus with multiple satellites is rare, long term follow-up is necessary to know how the lesion behaves.
| 1. |
Berlingeri-Ramos AC, Morales-Burgos A, Sánchez JL, Nogales EM. Spitz nevus in a hispanic population: A clinicopathological study of 130 cases. Am J Dermatopathol 2010;32:267-75.
[Google Scholar]
|
| 2. |
Zeng MH, Kong QT, Sang H, Deng DQ, Xie QM. Agminated spitz nevi: Case report and review of the literature. Pediatr Dermatol 2013;30:e104-5.
[Google Scholar]
|
| 3. |
Song JY, Kwon JA, Park CJ. A case of spitz nevus with multiple satellite lesions. J Am Acad Dermatol 2005;52 (2 Suppl 1):48-50.
[Google Scholar]
|
| 4. |
Zaenglein AL, Heintz P, Kamino H, Zisblatt M, Orlow SJ. Congenital spitz nevus clinically mimicking melanoma. J Am Acad Dermatol 2002;47:441-4.
[Google Scholar]
|
| 5. |
Urso C. A new perspective for spitz tumors? Am J Dermatopathol 2005;27;364-6.
[Google Scholar]
|
| 6. |
Kantrow S, Kalemeris GC, Prieto V. Spitz nevus with rosette-like structures: A new histologic variant. J Cutan Pathol 2008;35:510-2.
[Google Scholar]
|
Fulltext Views
3,461
PDF downloads
2,636





![[Figure - 1]](#fig_ijdvl_2015_81_1_96_148616_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2015_81_1_96_148616_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2015_81_1_96_148616_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2015_81_1_96_148616_f4.jpg){kind=link}