
Translate this page into:
Refractory moderate-to-severe pediatric-onset alopecia areata with elevated serum IgE treated by JAK inhibitors
Corresponding author: Dr. Hong Sang and Dr. Qingtao Kong, Department of Dermatology, Jinling Hospital, Nanjing Medical University, Nanjing, 210002, China. sanghong@nju.edu.cn; njukqt@163.com
-
Received: ,
Accepted: ,
How to cite this article: Wu Y, Deng L, Liu F, An B, Liu H, Sang H, et al. Refractory moderate-to-severe pediatric-onset alpecia areata with elevated serum IgEAb treated by JAK inhibitors. Indian J Dermatol Venereol Leprol. 2025;91:S35-S37. doi: 10.25259/IJDVL_849_2023
Dear Editor,
The management of refractory moderate-to-severe paediatric alopecia areata (AA) is challenging because of the high recurrence and ineffectiveness of the current therapeutic strategies. Although multiple therapeutic strategies have been explored in AA, no treatments have been completely effective. Baricitinib has been approved for the treatment of adult moderate-to-severe AA. However, the efficacy and safety of JAK inhibitors need to be evaluated in children.
Here, we report five cases of refractory moderate-to-severe paediatric-onset AA successfully treated either by baricitinib or tofacitinib. Refractory AA was defined as patients who had no response to standard therapies for at least 6 months, including minoxidil liniment, pilatory, oral glucocorticoids, enteric-coated thymopeptides, and Chinese medicines. Detailed medical information was obtained, and necessary laboratory tests were conducted to rule out contraindications (blood disorders, cancers, active infections, and a history of active tuberculosis, etc.) before the initiation of JAK inhibitors. These patients were treated with baricitinib 2 mg/day or tofacitinib 10 mg/day and underwent monthly follow-up. Since tofacitinib is more commonly used in children below 10 years than baricitinib, as per the previous reports, we preferred to choose tofacitinib in this age group.1 Two dermatologists assessed the severity of alopecia using the SALT (Scoring of Alopecia Tool) and AASIS (Alopecia Areata Symptom Impact Scale) scores at baseline and every month. Complete blood count, C-reactive protein, fasting lipid profile, liver and kidney functions, and blood coagulation tests were conducted for all patients at baseline and every 3 months during the treatment course. Serum IgE levels were determined in all patients before treatment using chemiluminescence assay (Siemens AG, Germany). Normal reference values for serum IgE were identified as follows: 1–5 years: 0–60 IU/mL, 6–9 years: 0–90 IU/mL, and 10–15 years: 0–200 IU/mL.
The characteristics of study patients have been summarised in Table 1. The age of onset ranged from 4 to 15 years, with a male-to-female ratio of 4:1, and all patients received JAK inhibitors (4 received tofacitinib, and 1 received baricitinib) for at least 6 months, with a median therapeutic course of 8 months (range 6–15 months). By the end of the study period, all five patients had achieved SALT 75 improvement, and 80% patients experienced 90% hair regrowth. Dynamic changes in SALT and AASIS scores from baseline and during the treatment are shown in [Figure 1]. Photos of the patients before and after treatment are shown in [Figure 2]. No significant adverse effects were observed during the administration. Two patients relapsed 7–10 days after the discontinuation of JAK inhibitors, but the condition ameliorated again after JAK inhibitors were resumed. Three patients had the tofacitinib dose reduced to 5mg/day after achieving cosmetically acceptable hair regrowth, as recommended by the physician, and no AA flares were observed during the following 2 to 3 months’ surveillance period. Around 80% of patients are still on therapy with JAK inhibitors and are followed up monthly.
| Case | Onset age(y)/gender/duration | body weight (kg) | Previous treatment | Allergic history | Accompanying disease | Treatment and course (m) | Adverse event | Initial SALT score | Latest SALT score | baseline IgE(IU/mL) |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 10/M/1 y | 46.5 | Minoxidil, Chinese medicine | N | N | Tofacitinib 5 mg BID, twice a day for 6 m, tapered to 5 mg QD, once a day for 2 m | N | 85 | 4 | 232 |
| 2 | 11/F/2 y | 48.5 | Minoxidil, Ciclosporin | N | CHD, thyroid nodule | Tofacitinib 5 mg BiD for 6 m | N | 88 | 55 | 57.5 |
| 3 | 4/M/4 y | 45 | Systemic glucocorticoids, ILCSs, Chinese medicine | Allergic rhinitis | N | Tofacitinib 5 mg BiD for 8 m, tapered to 5 mg QD for 3 m | Elevated liver transaminase | 100 | 10 | 200 |
| 4 | 10/M/5 y | 62.5 | Minoxidil liniment, thymopeptide capsule, pilatory | N | N | Baricitinib 2 mg QD for 8 m | N | 100 | 9 | >1130 |
| 5 | 15/M/6 m | 65 | Minoxidil liniment, Pilatory, Chinese medicine | N | N | Tofacitinib 5 mg BID for 15 m, tapered to 5 mg QD for 2 m | N | 100 | 0 | 25.7 |
M: male, F: female, y: year, m: month, N: none, CHD: congenital heart disease, ILCSs; Intralesional glucocorticosteroid.
Interestingly, we noted that 71.4% patients exhibited high serum IgE levels, which may contribute to the intractable and severity of the disease. Elevated serum IgE levels in AA have been elaborated in several studies, which were considered to be involved with Th2 immune responses.2 JAK inhibitors can reduce inflammation by preventing signal transduction and reduce the phosphorylation and activation of signal transduction and transcription factors (STAT) by blocking JAK. Furthermore, we noted that among the three patients, one exhibited a reduction in serum IgE levels within the normal range following 3 months of oral tofacitinib administration.
To date, only five reports including 59 cases documented baricitinib in paediatric AA. The majority of paediatric AA cases were treated with tofacitinib, with an estimated 95 cases from one prospective, single-centre study, one retrospective study, and case reports.3,4 Upadacitinib (2 cases), Ritlecitinib (105 cases), and Ruxolitinib (4 cases) were also prescribed in paediatric AA in previous reports. Hair regrowth was achieved in most patients after oral JAK inhibitors with an estimated efficiency of 88.21% (95% CI 88.13–88.29%).1 Adverse effects were mild and well tolerated. However, there is no long-term follow-up data on the treatment of JAK inhibitors in paediatric AA, and no standardised guidelines were formulated for the maintenance therapy and tapering of dosage.
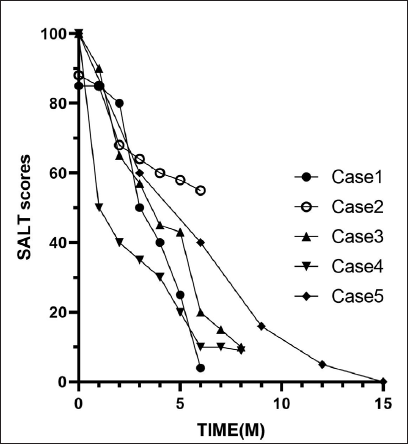
- All 5 patients had an improvement in the SALT scores throughout the treatment.
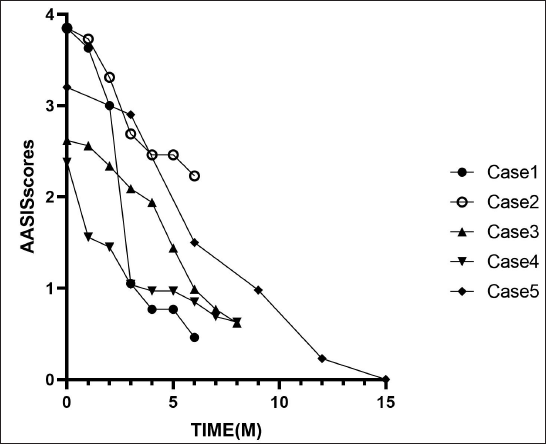
- All 5 patients had a decrease in AASIS scores throughout the treatment.
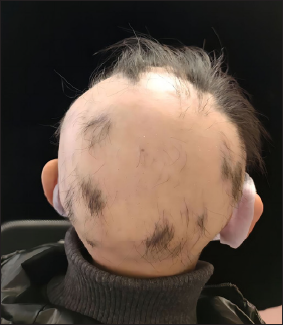
- Case 1 before treatment.

- After treatment of tofacitinib for 6 months, Case 1 showed rapid hair recovery and the SALT score decreased from 85 to 4.

- Case 2 before treatment.

- Case 2, an 11-year-old girl, achieved obvious hair regrowth after 6 months of tofacitinib treatment, with an improvement in the SALT score from 88 to 55.

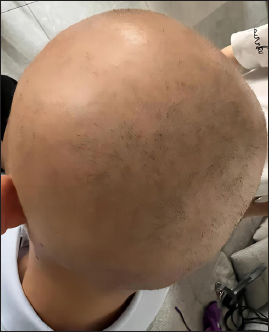
- Case 3 before treatment.

- After treatment of tofacitinib for 8 months, Case 3 showed significant hair recovery and the SALT score decreased from 100 to 10.
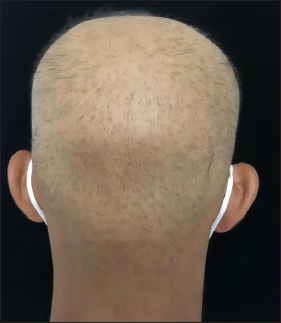
- Case 4 before treatment.

- Case 4 after 8 months of tofacitinib treatment showed an improvement in the SALT score from 100 to 9.
- Case 5 before treatment.

- Case 5 after treatment. He had a complete response after 15 months of baricitinib treatment.
A systematic review of tofacitinib in paediatric AA demonstrated an overall incidence rate of adverse events of 21%, most of which were mild and self-limiting.5 Therefore, JAK inhibitors have been considered to be promising agents with a low incidence of adverse events in the treatment of refractory paediatric AA. However, long-term surveillance studies with a larger sample size are required to evaluate the overall safety and adverse events in clinical settings.
Ethical approval
This study was approved by the Institutional Review Board of Jinling Hospital, Medical School of Nanjing University, Nanjing, number 2023DZGZR-055, dated 2023-03-10.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Special fund was received for the clinical research at Jinling Hospital [22LCYY-QH10].
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)–assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)–assisted technology for assistance in the writing or editing of the manuscript, and no images were manipulated using AI.
References
- Alopecia universalis in an adolescent successfully treated with upadacitinib-A case report and review of the literature on the use of JAK inhibitors in pediatric alopecia areata. Dermatol Ther (Heidelb). 2023;13:843-56.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Total serum immunoglobulin E in patients with alopecia areata. Indian Dermatol Online J. 2014;5:122-7.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Real-world experience and long-term evaluation of tofacitinib in refractory alopecia areata: A prospective, open-label, single-center study in Asian Arab population. Dermatol Ther. 2022;35:e15871.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of alopecia areata in pre-adolescent children with oral tofacitinib: A retrospective study. Pediatr Dermatol. 2021;38:103-8.
- [CrossRef] [PubMed] [Google Scholar]
- Oral surveillance and JAK inhibitor safety: The theory of relativity. Nat Rev Rheumatol. 2022;18:301-4.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]




