Translate this page into:
Reversal of pseudo-ainhum with acitretin in Camisa's syndrome
2 Acworth Municipal Hospital, Wadala, Mumbai, Maharashtra, India
Correspondence Address:
Mahendra M Kura
Department of Dermatology, Venereology and Leprosy,Grant Government Medical College, Mumbai - 400 008, Maharashtra
India
| How to cite this article: Kura MM, Parsewar S. Reversal of pseudo-ainhum with acitretin in Camisa's syndrome . Indian J Dermatol Venereol Leprol 2014;80:572-574 |
Sir,
Keratoderma hereditaria mutilans (KHM) or Vohwinkel′s syndrome is a type of cicatrizing palmoplantar keratoderma with autosomal dominant inheritance, first reported in 1929. [1] It is characterized by rugose keratoderma with a honeycomb pattern, starfish shaped keratotic plaques on the dorsum of hands and feet, and pseudo-ainhum at the interphalangeal joints. Its systemic associations include deaf-mutism, high tone acoustic impairment, spastic paraplegia, and ichthyosis. [2] Classical Vohwinkel′s syndrome is associated with deafness, but not with generalized ichthyosis. Camisa′s syndrome (variant Vohwinkel′s syndrome) is a rare variant which is associated with ichthyosis, but not with deafness. [3] Pseudo-ainhum is one of the classical features of this syndrome and is defined as a constricting circumferential band around a digit or limb. [4] We report the effectiveness of acitretin as a nonsurgical modality in the treatment of pseudo-ainhum in keratoderma associated with ichthyosis.
A 17-year-old unmarried girl, born of non-consanguineous marriage, complained of dark itchy, scaly lesions on her extremities and trunk along with thickening of palms and soles since early childhood. The severity of her skin lesions had increased with time, and she presented to us with large plate-like, polygonal, grey-brown, firmly adherent scales arranged in a mosaic pattern on the trunk, upper and lower extremities. The chest and neck showed rippled hyperkeratosis with extension to the shoulders bilaterally, with relative sparing of the face. There was history of winter exacerbation. Her palms and soles showed diffuse rugose keratoderma with transgrediens extending to the dorsum of hands and feet with sausage-like appearance of the digits. There were starfish-like keratotic plaques on the knuckles. Three years earlier, she had developed painful pus-filled lesions on her right fifth toe followed by gradual constriction at the base, ultimately progressing to auto-amputation. Subsequently, she developed a painful cicatricial band (pseudo-ainhum) at the base of her left fifth toe. At presentation, she had pseudo-ainhum at the left fifth metatarso-phalangeal joint (MTP) and narrow constrictions at other MTP joints [Figure - 1]. General and systemic examination were within normal limits. There was no history suggestive of collodion membrane at birth, blistering in early childhood, hearing or visual defects, seizures, mental retardation, or cicatricial alopecia. Past and personal history were not contributory. Similar skin lesions of lesser severity were present in two older brothers.
 |
| Figure 1: (a) Large plate-like polygonal brown adherent scales of lamellar icthyosis, (b) Cicatricial band at left fifth Metatarsophalangeal joint with loss of right fifth toe, (c) Transgredient keratoderma with sausage-like digits and starfish shaped keratotic plaques |
X-rays of her hands and feet revealed narrow soft tissue constriction at the base of the fifth left toe with normal bone and fracture with resorption of the right fifth toe. Routine blood investigations including lipid profile were within normal limits. Histopathology from an ichthyotic plaque showed laminated hyperkeratosis, parakeratosis and some foci of hypergranulosis suggestive of lamellar ichthyosis [Figure - 2]. Considering the presence of transgredient mutilating keratoderma with generalized lamellar ichthyosis in the absence of deafness, a diagnosis of variant Vohwinkel′s syndrome or Camisa′s syndrome was made.
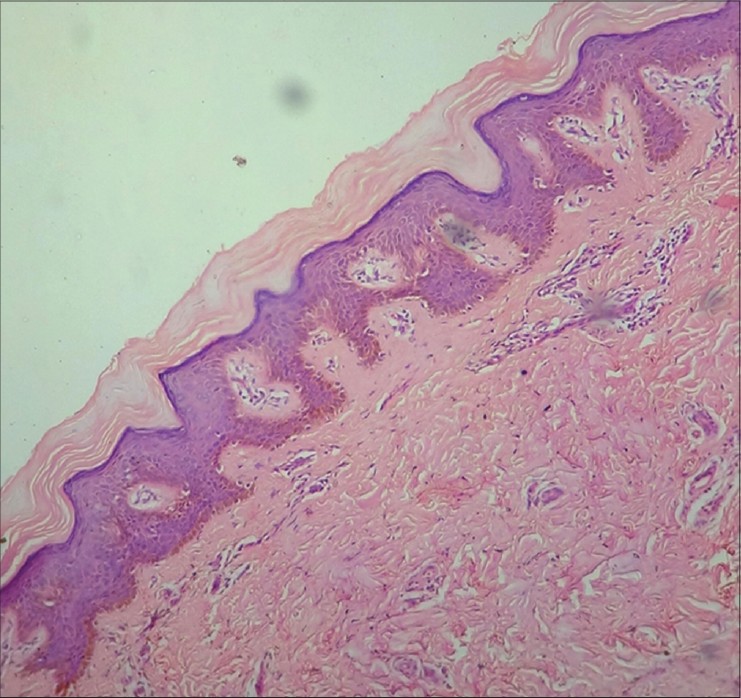 |
| Figure 2: HP (× 40) Laminated hyperkeratosis, parakeratosis, and hypergranulosis suggestive of lamellar ichthyosis |
After contraception counselling and a negative pregnancy test, the patient was started on oral acitretin 25 mg twice daily with monthy follow up for 6 months. While on treatment, there was complete reversal of pseudo-ainhum of the left fifth toe and significant improvement in the ichthyosis [Figure - 3] and [Figure - 4]. After stopping treatment for 1 year, the psedoainhum did not relapse; however, her ichthyosis relapsed with lesser severity.
 |
| Figure 3: (a and b) Before acitretin therapy showing ichthyotic scales and hyperkeratosis, (c and d) After acitretin therapy showing resolution of ichthyosis and hyperkeratosis |
 |
| Figure 4: (a) Before treatment with acitretin: Pseudo-ainhum of left fifth toe at Metatarso-phalangeal joint, (b) After 24 weeks of acitretin therapy showing improvement in pseudoainhum, (c) After 1 year showing complete reversal of pseudoainhum |
The term ainhum is applied to a painful constricting band, classically around the base of the fifth toe, in adults, which may involve only the skin, or may extend more deeply involving the fascia or bone, and can result in spontaneous amputation. It is most common in black Africans. Pseudo-ainhum is the term applied to other constricting bands around digits or limbs which may be congenital or secondary to other diseases like infection (particularly leprosy), recurrent trauma, cold injury, neuropathy (especially congenital sensory neuropathy), systemic sclerosis or chronic psoriasis. Pseudo-ainhum may also occur in association with certain hereditary diseases such as Vohwinkel′s palmoplantar keratoderma, pachyonychia congenita, erythropoietic protoporphyria, and Olmsted′s syndrome. [4] Vohwinkel′s mutilating keratoderma along with ichthyosis in the absence of deafness is termed Camisa′s syndrome, first reported by Camisa and Rossana. [3],[5] The types of ichthyoses associated with Camisa′s syndrome include ichthyosis vulgaris and lamellar ichthyosis (as seen in our case). [3],[5] The conventional treatment for pseudo-ainhum is surgery; in cases associated with keratinizing disorders, oral retinoids are helpful.
Acitretin, a monoaromatic second generation retinoid down regulates gene transcription leading to anti-proliferative, anti-inflammatory, and anti-keratinizing effects which are useful in various keratinizing diseases such as ichthyoses, keratodermas, psoriasis, Darier′s disease, and pityriasis rubra pilaris. There are previous reports of the utility of oral retinoids in the treatment of pseudo-ainhum. Rivers demonstrated the resolution of pseudo-ainhum associated with palmoplantar keratoderma with etretinate therapy. [6] Wereide found that oral etretinate brought about the disappearance of pseudo-ainhums and normalization of digital blood circulation in three patients with mutilating keratoderma. [7]
In our case, continuous treatment with acitretin for 6 months achieved a remarkable response in terms of near normalization of ichthyosis and reversal of pseudo-ainhum, ultimately preserving the toe. After discontinuing treatment for 1 year, the ichthyosis relapsed with lesser severity but pseudo-ainhum did not. To conclude, acitretin is a feasible, conservative, non-surgical, and durable therapeutic modality for the treatment of pseudo-ainhum-like mutilations associated with ichthyoses and mutilating keratodermas.
| 1. |
Vohwinkel KH. Keratoderma hereditarium meditans. Arch Dermatol Syphil 1929;158:354-64.
[Google Scholar]
|
| 2. |
Ali MM, Upadya GM. Variant of Vohwinkel's syndrome. Indian J Dermatol Venereol Leprol 2006;72:449-51.
[Google Scholar]
|
| 3. |
Rajashekar TS, Singh G, Naik CL, Okade R. Camisa disease: A rare variant of Vohwinkel's syndrome. Indian J Dermatol Venereol Leprol 2008;74:81.
[Google Scholar]
|
| 4. |
Burrows N, Lovell C. Disorders of connective tissue. In: Rook AJ, Burns T, Breathnach S, Cox N, Griffiths C editors. Textbook of Dermatology. 8 th ed, Vol 3. UK: Wiley-Blackwell Science Ltd; 2010. p. 69-70.
[Google Scholar]
|
| 5. |
Camisa C, Rossana C. Variant of keratoderma hereditaria mutilans (Vohwinkel's syndrome). Treatment with orally administered isotretinoin. Arch Dermatol 1984;120:1323-8.
[Google Scholar]
|
| 6. |
Rivers JK, Duke EE, Justus DW. Etretinate: Management of keratoma hereditaria mutilans in four family members. J Am Acad Dermatol 1985;13:43-9.
[Google Scholar]
|
| 7. |
Wereide K. Mutilating palmoplantar keratoderma successfully treated with etretinate. Acta Derm Venereol 1984;64:566-9.
[Google Scholar]
|
Fulltext Views
5,583
PDF downloads
1,444





![[Figure - 1]](#fig_ijdvl_2014_80_6_572_144220_u1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2014_80_6_572_144220_u2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2014_80_6_572_144220_u3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2014_80_6_572_144220_u4.jpg){kind=link}