Translate this page into:
Second to fourth digit ratio in female patients with acne vulgaris: Could it be a predictor of androgen receptor status?
2 Department of Pathology, Faculty of Medicine, Menoufia University, Al Minufya, Egypt
3 Department of Clinical Pharmacy, Faculty of Pharmacy, MSA University, October City, Egypt
Correspondence Address:
Azza Gaber Antar Farag
Department of Dermatology, Andrology and STDs, Faculty of Medicine, Menoufia University, Shibin El-Kom, El Menoufia
Egypt
| How to cite this article: Farag AG, Shoiab MA, Samaka R, Abdou AG, Elnaidany NF, Mansour AO. Second to fourth digit ratio in female patients with acne vulgaris: Could it be a predictor of androgen receptor status?. Indian J Dermatol Venereol Leprol 2019;85:590-596 |
Abstract
Background: Second to fourth digit (2D:4D) ratio is the ratio of index to ring fingers length. It reflects prenatal androgen exposure and sensitivity. Androgens are important in the pathogenesis of acne vulgaris, This ratio may therefore be of significance in determining the expression of androgen receptors.
Aim: To investigate the relationship between second to fourth digit ratio and androgen receptor expression in female patients with acne vulgaris and to assess its association with clinical aspects of acne vulgaris.
Methods: Females patients (n = 352) with different degrees of acne vulgaris severity and 168 age-matched females were enrolled. Right, left and total second to fourth digit ratios were calculated. Biopsies from all participants were processed for androgen receptor expression by immunohistochemical method.
Results: Right, left and total second to fourth digit ratios were significantly lower in acne vulgaris patients than controls (P < 0.001 for all), and each of them had a significant negative correlation with duration of acne vulgaris (P < 0.001; P = 0.013; P < 0.001, respectively). Androgen receptors were detected in epidermal keratinocytes, hair follicles, sebaceous glands and fibroblasts. Right second to fourth digit ratio showed a negative correlation with androgen receptor H score of keratinocytes (r = −0.28;P = 0.02), hair follicles (r = −0.22; P = 0.05) and fibroblasts (r= −0.37;P = 0.001), while left second to fourth digit ratio demonstrated negative correlation with androgen receptor H score of sebocytes (r = −0.397; P < 0.000) only.
Limitations: Lack of follow-up and absence of male participants were the main limitations of this study.
Conclusion: A masculine second to fourth digit ratio in female patients could anticipate acne vulgaris development, its duration and severity. Moreover, this ratio is associated with an upregulation of cutaneous androgen receptors. Taken together, second to fourth digit ratio could help in designing plans for treatment of acne vulgaris.
Introduction
Acne vulgaris is a chronic multifactorial inflammatory disease of the pilosebaceous unit.[1] It is characterized by androgen-induced excess sebum production, follicular hyperkeratinization, inflammation and altered adaptive immune response.[2] Presence of high androgen levels is important for the development of acne lesions. However, majority of acne patients exhibit normal levels of circulating androgens, suggesting that the impact of androgens on development of acne lesions might be related to end-organ sensitivity.[3],[4]
Androgen receptor is a nuclear steroid hormone receptor that has three binding domains: DNA binding domain, ligand binding domain and N-terminal regulatory domain. Like other steroid receptors, androgen receptor exists in the cytoplasm, in polymeric complexes. Upon binding to its ligand, for example, testosterone, it is trans-located into the nucleus and binds to androgen response elements and acts as the promotor of androgen-regulated genes to upregulate their expression.[5] Actually, regulation of androgen receptor function is controlled by both androgens and androgen receptor co-regulators.[6] More than 200 androgen receptor co-regulators have been identified, including transcription factors (e.g. activator protein 1), chaperones (e.g. heat shock protein 70) and kinases (e.g. male germ cell-associated kinase).[5],[6]
In acne, androgen receptors enhance fibroblast growth factor receptor 2 activity, which has a critical role in the development and homeostasis of sebaceous glands. It might also increase the expression of sterol regulatory element binding proteins that enhances lipogenesis in sebocytes.[7] Furthermore, genetic polymorphisms, such as short cytosine–adenine–guanine repeats in androgen receptor genes increase androgen sensitivity, and are more prevalent in people with acne vulgaris.[8] Androgens/androgen receptor interaction enhances inflammatory responses of macrophages and neutrophils. Moreover, androgen activity is associated with insulin-like growth factor-1 in regulating acne development.[7]
Ratio of second to fourth digit is the ratio of length of second finger (index finger) to fourth finger (ring finger). This ratio is fixed at an early age and remains relatively stable across the lifespan.[9] Generally, men have a longer ring relative to the index fingers, explaining a low second to fourth digit ratio.[10],[11],[12],[13],[14] In animal experiments, masculine second to fourth digit ratio was observed in the offspring of pregnant rats exposed to a high level of testosterone.[11],[15] A masculine ratio is associated with congenital adrenal hyperplasia in both boys and girls.[16],[17] High digit ratio (feminine ratio) is reported in androgen insensitivity syndrome in men (XY), indicating the importance of end-organ sensitivity.[18],[19] Furthermore, single-nucleotide gene polymorphism in androgen receptor with a low cytosine–adenine–guanine repeats, androgen-sensitive gene, has been reported to correlate with low second to fourth digit ratio.[13] Prenatal androgen peak, between 13 and 15 weeks of gestation, affects development of both sebaceous gland and digits,[20] a role that may indicate the association of acne vulgaris with the second to fourth digit ratio.[21] Although the role of androgen receptor is already established in both acne pathogenesis [8] and digit development,[13] the relationship of second to fourth digit ratio and androgen receptor in acne patients has not yet been investigated.
Therefore, we aimed to investigate the relationship between second to fourth digit ratio and androgen receptor status in acne lesions in female patients and to assess its association with clinical aspects (age of onset, duration and/or severity) of the disease.
Materials and Methods
This was a cross-sectional study of female patients (n = 352, ≥16 years old) with different degrees of acne vulgaris severity, controlled to age-matched acne-free healthy volunteer females (n = 168) from biorepository banking services who agreed supporting our research. Cases were recruited from a tertiary health care provider in dermatology clinic at Menoufia University Hospitals, Shebin El-Kom, El Menoufia, Egypt, during the period between January 2015 to October 2016, following institutional approval of the study by the Ethics Committee, Faculty of Medicine, Menoufia University, Egypt in accordance with the Helsinki declaration, 1975 (revised in 2000). An informed consent was signed before enrolling into this study. We excluded subjects with a history of injury and/or illness that could have lead to deformities of fingers, as well as those with a history of drugs that could induce acne. Double-blind randomization was followed up to the end of the study. Study coordinator disclosed the patient identification, to link lab results, and for classification of patients groups for statistical analysis and results tabulation.
Each participant in this study was subjected to a thorough medical history and physical examination to apply the inclusion/exclusion criteria. Dermatological examination was performed using the International Consensus Conference on acne classification system, to confirm acne diagnosis and grade its severity.[22] Mild acne presented with comedones and papules. Moderate acne was distinguished by several papules, pustules and some nodules. Severe acne was characterized by numerous or extensive papules–pustules or both, along with many nodules. Very severe forms of acne included acne conglobata and acne fulminans.
Second to Fourth Digit Ratio
For all participants in the study, the lengths of second and fourth fingers were measured using a digital caliper with a resolution of 0.01 mm. Finger length was measured on the palmar side of the hand from the basal meta-carpo-phalangeal crease or, if more than one, from the most proximal crease to the fingertip in both right and left hands. Finger lengths were evaluated before assessment of acne to eliminate inter-observer measurement differences. The second to fourth digit ratio was obtained by dividing the length of second finger by fourth finger's length, for both right and left hand, and the average of both hands was calculated to represent the total second to fourth digit ratio. So, for each participant right, left and total second to fourth digit ratios were calculated, as described in a previous studyr.[13]
Skin biopsy and immunohistochemical staining
From the back of all participants, 2 mm punch skin biopsies were taken. From each biopsy, multiple 4 μm thickness sections were cut. Slides were subjected to subsequent steps of deparaffinization and rehydration. Antigen retrieval was performed by boiling in citrate buffer saline (pH 6) for 20 min, followed by cooling at room temperature. Endogenous peroxidase activity was blocked by incubation with 6% H2O2 in methanol. The primary antibody [mouse monoclonal antibody against androgen receptor (Clone AR441) at 1:50 dilution] (LabvVsion ®, Neomarker, CA, USA) was incubated overnight at room temperature. Immunoreactivity for androgen receptor was visualized using Envision system (Dako ®, Copenhagen, Denmark) with DAB chromogenic substrate and Mayer's hematoxylin as a counter stain. Negative control was prepared by substituting the primary antibody with cross-matched isotopes. Normal prostate was used as a positive tissue control. Specimen was considered androgen receptor positive if more than 1% of cells showed nuclear immunoreactivity. Evaluation of intensity and percentage of immunoreactivity was done, after which H score formula (H score = mild intensity (1) × percentage + moderate intensity (2) × percentage + strong intensity (3) × percentage) was calculated and reported for every specimen.
Statistical analysis
Data of this study was collected and processed on IBM-PC compatible computer using SPSS software version 20.0 (SPSS Inc., Chicago, USA). Student's t-test and Mann–Whitney U-test were used to compare quantitative data according to its distribution. Chi-square test was used for qualitative data and Spearman correlation to assess correlations. P < 0.05 was considered as the cut-off value for significance.
Results
The demographic and clinical data of studied subjects
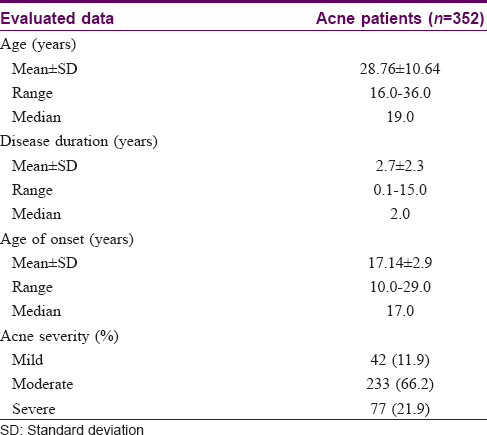
The present study included 352 female acne patients, their age ranging from 16 to 36 years with 19 years as a median value and 28.76 ± 10.64 as a mean ± SD. The controls were 168, age-matched (20.34 ± 4.812 years) acne-free healthy female volunteers.
Clinical data of the acne patient group are presented in [Table - 1].
Second to fourth digit ratios of studied subjects
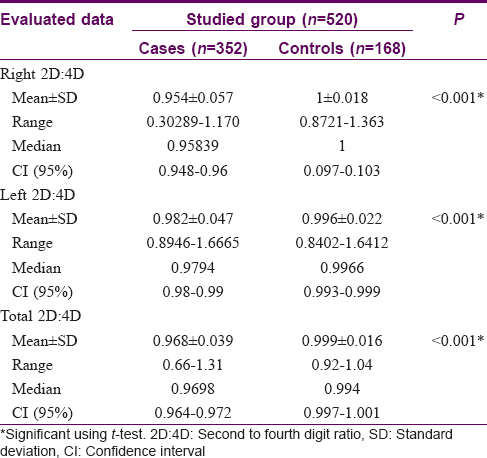
Compared with controls, patients had significant (P < 0.001) decrease in their right (0.954 ± 0.057 vs 1 ± 0.018), left (0.982 ± 0.047 vs 0.996 ± 0.022) and total (0.968 ± 0.039 vs 0.999 ± 0.016) second to fourth digit ratios [Table - 2].
Second to fourth digit ratios and clinical parameters in acne patients
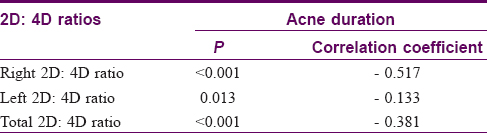
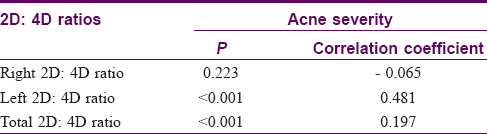
There were significant negative correlations between the duration of acne vulgaris and second to fourth digit ratio in each hand (right, P < 0.001, r = −0.517, [Table - 3] and left, P = 0.013, r = −0.133, [Table - 3]) separately and their total mean values (P < 0.001, r = −0.381) [Table - 3]. However, insignificant correlations were recorded regarding age of onset of acne lesions (P > 0.05). Concerning severity of acne vulgaris, left [Table - 4] and total [Table - 4] second to fourth digit ratio showed significant positive correlation (P < 0.001, r = 0.481; P< 0.001, r = 0.197, respectively) with acne severity, while right second to fourth digit ratio revealed nonsignificant negative correlation (r = −0.065, P = 0.223).
Androgen receptor expression
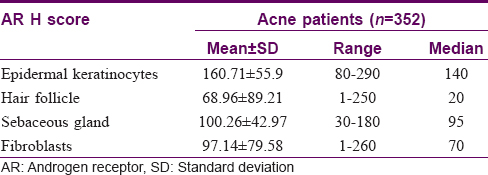
In acne vulgaris cases, androgen receptor expression was positive in all examined cases (n = 352) (100%) and showed moderate-to-strong degree of intensity. This receptor exhibited positive immunoreactivity in epidermal keratinocytes [Figure - 1]a and dermal cellular elements, including hair follicles [Figure - 1]b, sebaceous glands [Figure - 1]c and fibroblasts [Figure - 1]d. H score of androgen receptor expressions in positive cutaneous elements was demonstrated in [Table - 5].
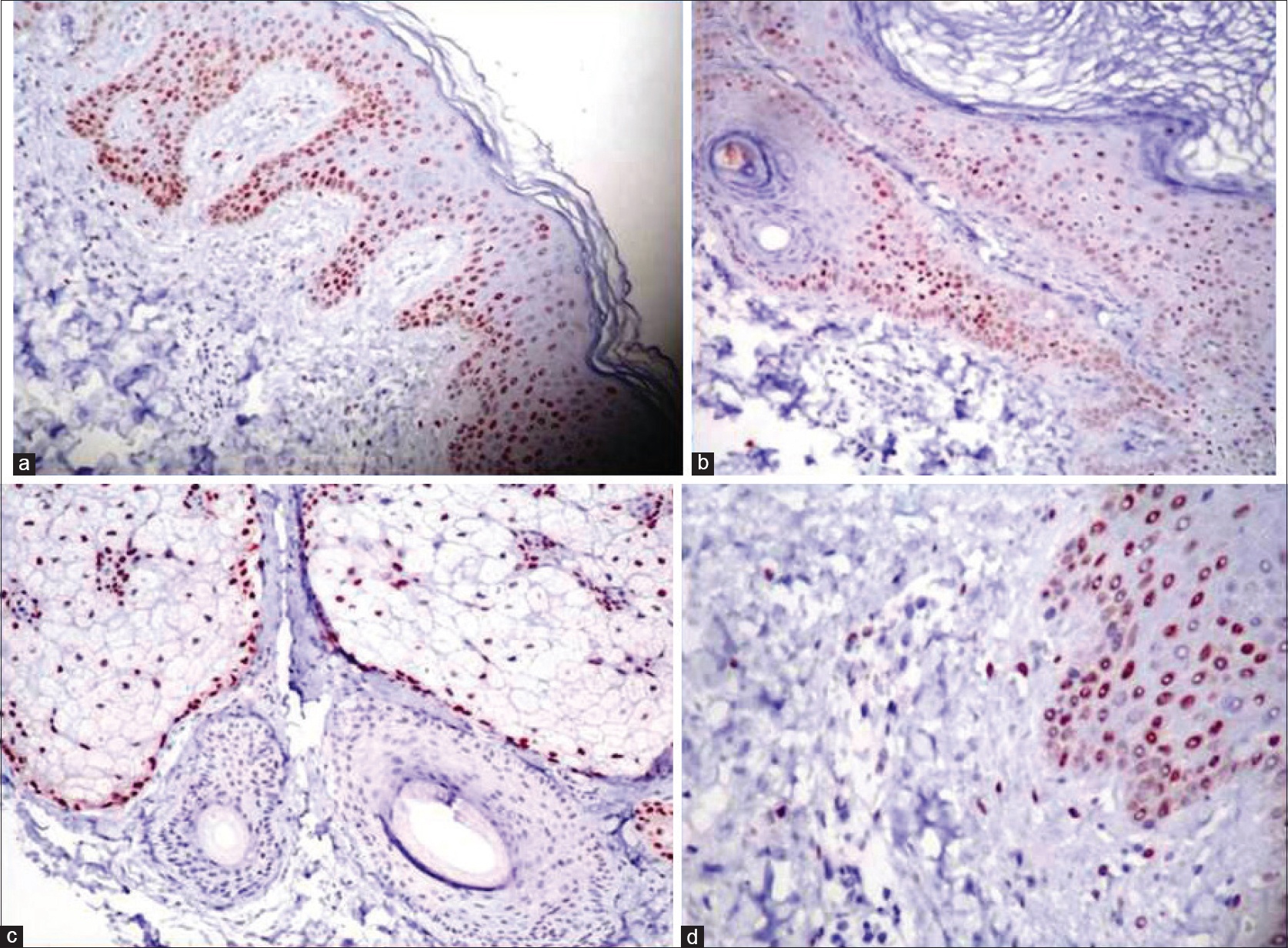 |
| Figure 1: Nuclear immunoreactivity of androgen receptor (mouse monoclonal antibody; Clone AR441) in (a) epidermis of acne vulgaris biopsies (immunohistochemistry, ×100); (b) hair follicles of acne vulgaris biopsies (immunohistochemistry × 100); (c) sebaceous glands of acne vulgaris biopsies (immunohistochemistry, ×100); (d) epidermis as well as fibroblasts of acne vulgaris biopsies (immunohistochemistry, ×100) |
In controls, androgen receptor immunoreactivity was seen in the cytoplasm of 80% of the examined cases which was considered as artefactual (i.e. negative).[23]
Association of second to fourth digit ratio with H score of androgen receptor expressions in acne patients
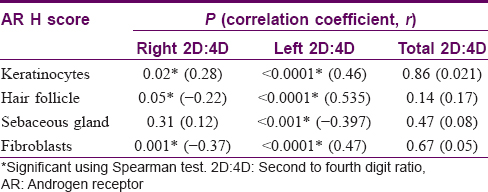
Right second to fourth digit ratio negatively correlated with androgen receptor H score mean values of keratinocytes (r = −0.28; P = 0.02), hair follicles (r = −0.22; P = 0.05) and fibroblasts (r = −0.37; P = 0.001). However, left second to fourth digit ratio demonstrated negative correlation with H score of sebocytes (r = −0.397; P= 0.000), but positive correlation regarding H score of keratinocytes (r = 0.46; P = 0.000), hair follicles (r = 0.535; P= 0.000) and fibroblasts (r = 0.47; P = 0.000). On the contrary, the total second to fourth digit ratio showed insignificant correlation with any of assessed H score mean values (P > 0.05 for all) [Table - 6].
Discussion
To verify the prenatal androgen role in acne pathogenesis in females, we evaluated second to fourth digit ratio in each hand (right and left) separately, as well as their total mean value in 352 female patients with acne vulgaris compared to 168 controls, who were females without acne. We have earlier studied second to fourth digit ratio in 169 male patients with acne vulgaris vs. 63 healthy volunteer males. We observed insignificant difference between cases and controls regarding right, left and total second to fourth digit ratios (data not published). In view of this, all our selected subjects were females. We were unable to find any previous reports demonstrating the relationship between second to fourth digit ratio and androgen receptor expression simultaneously in acne patients. Therefore, this study may be the first one dealing with this issue.
In agreement with the results of Bilgiç et al., in our study, female patients with acne demonstrated significant decrease in right, left and total second to fourth digit ratios when compared to their matched peers.[21] Zouboulis et al. detected an increased sebum secretion in adult female rats that were exposed to androgens in the first week of their fetal life.[24] This suggests that female fetuses exposed to higher androgens are at higher risk of developing acne., Second to fourth digit ratio is different in males and females and thus could be used as a predictor of development of acne vulgaris in females.
On the contrary, Unal et al. reported an insignificant decrease in second to fourth digit ratios (right, left and total) in female acne patients compared with their matched controls.[25] However their sample size was small (91 patients).
Surprisingly, we found a positive correlation between acne severity with both left and total second to fourth digit ratios in our cases i.e. feminine second to fourth digit ratio is associated with severe acne in females, indicating that acne vulgaris is a multifactorial disease and reasons other than androgens may account for acne severity. Absence of significant correlation between acne severity and the clinical or laboratory androgenicity indicators was also reported in another study.[26]
However, in the right hand, second to fourth digit ratio showed a negative correlation with acne severity (r = −0.065); although this correlation could not reach the level of significance (P = 0.223). This supports the result of an earlier study in which the authors reported that the right second to fourth digit ratio had stronger relationship with fetal testosterone than the left ratio, suggesting that the right hand is more sensitive to prenatal sex androgens than the left.[27]
Regarding duration of acne, we observed that masculine second to fourth digit ratio is more prevalent in those suffering from a longstanding acne, indicated by negative correlation of all second to fourth digit ratios (right, left and total) and acne vulgaris disease duration. However, Bilgiç et al. reported a negative correlation between the duration of acne and right second to fourth digit ratio only.[21] On the contrary, Unal et al. demonstrated a significant positive correlation between disease duration and left and total digit ratios.[25] These differences could be possibly explained by the small sample size in the latter. study.[25] Moreover, there could have been a possible selection bias in their study, based on selection of patients seeking for medical advice only.[25]
Androgen receptor expression is of utmost significant importance in acne pathogenesis,[23] supported by androgen-independent androgen receptor activation through its co-regulators.[7] As reported earlier also, we demonstrated androgen receptor expression in epidermal and follicular keratinocytes, sebocytes and dermal fibroblasts.[13] Moreover, we observed positive androgen receptor immunoreactivity in all our acne patients. However, Durusoy et al.[28] in Germany reported androgen receptor positivity in 78.8% of their evaluated acne cases while lower positivity (55%) was recorded in India.[23] This difference in androgen receptor expression could be attributed to small sample size (n = 20) in the latter study, and/or could be genetically explained.[23]
Parallel to its observed role in predicting acne development in females, second to fourth digit ratio could also predict expression of androgen receptors in acne vulgaris skin, indicated by the demonstrated significant correlation between right and left second to fourth digit ratios and androgen receptor H score mean values in acne skin biopsies in our study.
Recently, Pakhiddey et al. reported that, in acne vulgaris patients, androgen receptor expression may be used to predict clinical response to acne treatment and may be used to plan the treatment of acne vulgaris.[23] Androgen receptor evaluation necessitates skin biopsy, which is an invasive procedure usually not accepted by acne patients. However, from the present study, we recommend evaluation of second to fourth digit ratio as a noninvasive simple tool, to give an idea about the cutaneous androgen receptor load in female acne patients, which could subsequently be taken as a base parameter in planning treatment.
In this study, the focus was only on female patients with acne vulgaris. Absence of male participants and lack of follow-up were the limitations of the current study. Further studies will be needed to examine masculine second to fourth digit ratio in both male and female acne patients and response to different treatment modalities on cutaneous androgen receptor expression.
Conclusion
Based on aforementioned findings, we confirmed the role of second to fourth digit ratio as a predictor for development of acne vulgaris, its severity, and disease duration in female patients. Additionally, it may be considered as an indirect measurement of androgen receptor status, and could be taken as a basal clinical parameter in planning treatment for acne.
Acknowledgement
The authors are grateful to Dr. Sally Mohsin, Department of Public Health and Community Medicine, Faculty of medicine-Menoufia University, Egypt, for helping in the statistical analysis of this study.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patients have given their consent for their images and other clinical information to be reported in the journal. The patient understands that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Webster GF. The pathophysiology of acne. Cutis 2005;76:4-7.
[Google Scholar]
|
| 2. |
Dawson AL, Dellavalle RP. Acne vulgaris. BMJ 2013;346:f2634.
[Google Scholar]
|
| 3. |
Zouboulis CC. Acne vulgaris. The role of hormones. Hautarzt 2010;61:107-8, 110-4.
[Google Scholar]
|
| 4. |
Kurokawa I, Danby FW, JU Q, Wang X, Xiang LF, Xia L, et al. New developments in our understanding of acne pathogenesis and treatment. Exp Dermatol 2009;18:821-32.
[Google Scholar]
|
| 5. |
Van de Wijngaart DJ, Dubbink HJ, Van Royen ME, Trapman J, Jenster G. Androgen receptor co regulators: Recruitment via the co activator binding groove. Mol Cell Endocrinol 2012;352:57-69.
[Google Scholar]
|
| 6. |
Heemers HV, Tindall DJ. Androgen receptor (AR) coregulators: A diversity of functions converging on and regulating the AR transcriptional complex. Endocr Rev 2007;28:778-808.
[Google Scholar]
|
| 7. |
Lai JJ, Chang P, Lai KP, Chen L, Chang C. The role of androgen and androgen receptor in skin-related disorders. Arch Dermatol Res 2012;304:499-510.
[Google Scholar]
|
| 8. |
Pang Y, He CD, Liu Y, Wang KB, Xiao T, Wang YK, et al. Combination of short CAG and GGN repeats in the androgen receptor gene is associated with acne risk in North East China. J Eur Acad Dermatol Venereol 2008;22:1445-51.
[Google Scholar]
|
| 9. |
McIntyre MH, Ellison PT, Lieberman DE, Demerath E, Towne B. The development of sex differences in digital formula from infancy in the Fels Longitudinal Study. Proc Biol Sci 2005;272:1473-9.
[Google Scholar]
|
| 10. |
Breedlove SM. Minireview: Organizational hypothesis: Instances of the fingerpost. Endocrinology 2010;151:4116-22.
[Google Scholar]
|
| 11. |
Chai XJ, Jacobs LF. Digit ratio predicts sense of direction in women. PLoS One 2012;7:e32816.
[Google Scholar]
|
| 12. |
Hönekopp J, Watson S. Meta-analysis of digit ratio 2D:4D shows greater sex difference in the right hand. Am J Hum Biol 2010;22:619-30.
[Google Scholar]
|
| 13. |
Manning JT, Bundred PE, Newton DJ, Flanagan BF. The second to fourth digit ratio and variation in the androgen receptor gene. Evol Hum Behav 2003;24:399-405.
[Google Scholar]
|
| 14. |
Manning JT. Resolving the role of prenatal sex steroids in the development of digit ratio. Proc Natl Acad Sci U S A 2011;108:16143-4.
[Google Scholar]
|
| 15. |
Talarovicová A, Krsková L, Blazeková J. Testosterone enhancement during pregnancy influences the 2D: 4D ratio and open field motor activity of rat siblings in adulthood. Horm Behav 2009;55:235-9.
[Google Scholar]
|
| 16. |
Okten A, Kalyoncu M, Yariş N. The ratio of second- and fourth-digit lengths and congenital adrenal hyperplasia due to 21-hydroxylase deficiency. Early Hum Dev 2002;70:47-54.
[Google Scholar]
|
| 17. |
Brown WM, Hines M, Fane BA, Breedlove SM. Masculinized finger length patterns in human males and females with congenital adrenal hyperplasia. Horm Behav 2002;42:380-6.
[Google Scholar]
|
| 18. |
Berenbaum SA, Bryk KK, Nowak N, Quigley CA, Moffat S. Fingers as a marker of prenatal androgen exposure. Endocrinology 2009;150:5119-24.
[Google Scholar]
|
| 19. |
Minto CL, Liao KL, Conway GS, Creighton SM. Sexual function in women with complete androgen insensitivity syndrome. Fertil Steril 2003;80:157-64.
[Google Scholar]
|
| 20. |
Zouboulis CC. Acne and sebaceous gland function. Clin Dermatol 2004;22:360-6.
[Google Scholar]
|
| 21. |
Bilgiç Ö, Doǧdu M, İslamoǧlu GK, Altınyazar C. The relationship between the second to fourth digit ratio and acne vulgaris. J Eur Acad Dermatol Venereol 2014;28:1340-3.
[Google Scholar]
|
| 22. |
Pochi PE, Shalita AR, Strauss JS, Webster SB, Cunliffe WJ, Katz HI, et al. Report of the consensus conference on acne classification. Washington, D.C. March 24 and 25, 1990. J Am Acad Dermatol 1991;24:495-500.
[Google Scholar]
|
| 23. |
Pakhiddey R, Paul S, Mandal AK, Kumar V. Epidermal androgen receptors in acne vulgaris patients before and following oral isotretinoin. J Anat Soc India 2015;64:42-7.
[Google Scholar]
|
| 24. |
Zouboulis CC, Fimmel S, Ortmann J, Turnbull JR, Boschnakow A. Sebaceous glands. In: Hoath SB, Maibach HI, editors. Neonatal Skin: Structure and Function. 2nd ed. New York: Marcel Dekker; 2003. p. 59-87.
[Google Scholar]
|
| 25. |
Unal M, Urun Unal G, Balevi S, Tol H, Uyar M. The second to fourth digit ratio in acne vulgaris. Pediatr Dermatol 2015;32:651-5.
[Google Scholar]
|
| 26. |
Cibula D, Hill M, Vohradnikova O, Kuzel D, Fanta M, Zivny J, et al. The role of androgens in determining acne severity in adult women. Br J Dermatol 2000;143:399-404.
[Google Scholar]
|
| 27. |
Manning JT, Scutt D, Wilson J, Lewis-Jones DI. The ratio of 2nd to 4th digit length: A predictor of sperm numbers and concentrations of testosterone, luteinizing hormone and estrogen. Hum Reprod 1998;13:3000-4.
[Google Scholar]
|
| 28. |
Durusoy C, Alpsoy E, Elpek O, Karpuzoglu G. Androgen receptor levels in the sebaceous glands of papulopustular lesions from patients with Behçet's disease and acne vulgaris: A controlled study. Adv Clin Path 2002;6:87-93.
[Google Scholar]
|
Fulltext Views
4,717
PDF downloads
2,313





![[Table - 1]](#tbl_ijdvl_2019_85_6_590_261209_t2.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2019_85_6_590_261209_t3.jpg){kind=link}
![[Table - 3]](#tbl_ijdvl_2019_85_6_590_261209_t4.jpg){kind=link}
![[Table - 4]](#tbl_ijdvl_2019_85_6_590_261209_t5.jpg){kind=link}
![[Figure - 1]](#fig_ijdvl_2019_85_6_590_261209_f1.jpg){kind=link}
![[Table - 5]](#tbl_ijdvl_2019_85_6_590_261209_t6.jpg){kind=link}
![[Table - 6]](#tbl_ijdvl_2019_85_6_590_261209_t7.jpg){kind=link}