Translate this page into:
Serpentine supravenous hyperpigmentation induced by docetaxel
Correspondence Address:
Anupam Das
"Prerana", 19, Phoolbagan, Kolkata 700 086, West Bengal
India
| How to cite this article: Das A, Kumar D, Mohanty S, Mondal AK, Chowdhury SN, Bandyopadhyay D. Serpentine supravenous hyperpigmentation induced by docetaxel. Indian J Dermatol Venereol Leprol 2015;81:434 |
Sir,
Serpentine supravenous hyperpigmentation (SSH) was the term coined by Hrushesky to describe increased pigmentation of the skin immediately overlying the venous network used for intravenous infusion of 5-fluorouracil. [1] Subsequently, this phenomenon has been observed in individuals treated with other chemotherapeutic agents as well. The terms "persistent supravenous erythematous eruption" (PSEE), "persistent serpentine supravenous hyperpigmented eruption" (PSSHE), and "persistent serpentine supravenous hyperpigmentation" have been used to describe this condition. It begins as red streaks commonly over the injected veins, followed by hyperpigmentation. The condition is benign and self-limiting. [2] We describe a patient who developed linear serpentine erythematous eruption overlying the superficial veins after treatment with intravenous docetaxel for breast carcinoma.
A 72-year-old man was diagnosed with operable infiltrating duct carcinoma of the left breast with lymph node positivity. Subsequently, he was put on adjuvant chemotherapy with docetaxel, doxorubicin, and cyclophosphamide (TAC regimen), cycled 3 weekly for 6 weeks. He was pre-medicated with ondansetron, 8 mg twice daily, dexamethasone, 8 mg twice daily, pantoprazole, 40 mg, and chlorpheniramine. Docetaxel in the dose of 100 mg/m 2 was administered in a 250-ml polyvinyl chloride-free sodium chloride 0.9% bag over 1 hour. After receiving his first dose of docetaxel infusion along the left lower limb, he experienced severe pain around the injection site which subsided spontaneously in 2 days. Following this, he noticed a red line spreading along the path of infusion of the drug. The erythematous line was subsequently replaced by dark-colored streaks [Figure - 1]. The next doses of the drug (100 mg/m 2 in a 250 ml polyvinyl chloride-free sodium chloride 0.9% bag over 1 hour) were subsequently administered along the veins of the right and left forearms and a similar clinical course of events was noticed. [Figure - 2] and [Figure - 3] Cutaneous examination revealed linear streaks of hyperpigmentation along the tributaries of long saphenous vein of left lower limb and also along the veins over the extensor aspect of left forearm. Some vesicles were also noted over the cephalic vein of right forearm. The veins underlying the pigmented streaks were neither tender nor thickened. There was no regional lymphadenopathy. Examination of the palms, soles, and mucous membrane was unremarkable. Complete hemogram and routine biochemistry panel were normal. Histopathological examination of a biopsied specimen of the involved skin revealed basal layer degeneration, pigment incontinence, melanophages, focal band-like infiltrate as well as perivascular mononuclear infiltrate. [Figure - 4] Based on the clinical pattern and histopathological features, a diagnosis of docetaxel-induced supravenous serpentine dermatitis was made. The patient was prescribed topical steroids and emollients. Venous washing was not done in any of the instances.
 |
| Figure 1: Linear streak of hyperpigmentation along the tributaries of long saphenous vein of left lower limb |
 |
| Figure 2: Linear streak of hyperpigmentation along the venous prominences in left forearm |
 |
| Figure 3: Hyperpigmentation along with vesicles over the cephalic vein of right upper limb |
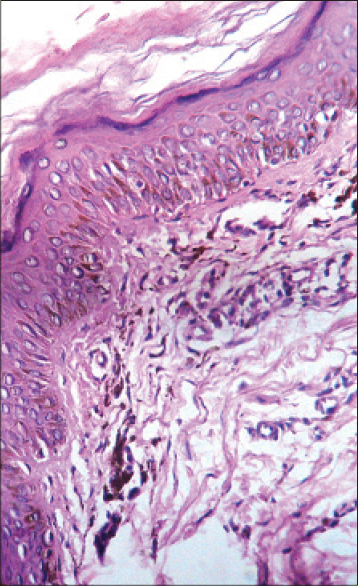 |
| Figure 4: Basal layer degeneration, pigment incontinence, melanophages, and band like infiltrate (H and E; ×40) |
Supravenous serpentine hyperpigmentation is a rare sequel of infusion of many anti-cancer drugs such as nitrogen mustard, cyclophosphamide, actinomycin, doxorubicin, vinca alkaloids, taxanes, and bortezomib. [2] The exact mechanism of pigment induction is unknown but it has been postulated that these cytotoxic drugs cause loss of integrity of vascular endothelium. This leads to leakage of the drug from the vessel to the overlying epidermis leading to hyperpigmentation. [3] According to another school of thought, the offending drug accumulates within the skin overlying the blood vessels which may induce a localized and sometimes generalized hypersensitivity reaction. [4],[5]
Histopathologically, the condition may show interface dermatitis with isolated necrotic keratinocytes, papillary dermal edema, and superficial perivascular inflammatory infiltrates. Based on the morphology of the lesion, the clinical differential diagnosis should include thrombophlebitis, cutis marmorata, erythema ab igne, livedo reticularis, and lichen planus running along superficial cutaneous veins. [6] The underlying vessels of serpentine supravenous hyperpigmentation remain patent and non-tender unlike thrombophlebitis where the underlying vein is occluded by blood clot and is tender. [7] The above mentioned differential diagnoses can be readily excluded by thorough history taking and proper clinical examination. Physicians should be aware of this cutaneous side effect of cytotoxic agents owing to their widespread use in the treatment of malignancies. Topical application of corticosteroids has been found to be beneficial. [2]
| 1. |
Hrushesky WJ. Letter: Serpentine supravenous fluorouracil hyperpigmentation. JAMA 1976;236:138.
[Google Scholar]
|
| 2. |
Ghosh SK, Bandyopadhyay D, Ghoshal L, Basu S. Letter: Docetaxel-induced supravenous serpentine dermatitis. Dermatol Online J 2011;17:16.
[Google Scholar]
|
| 3. |
Jain V, Bhandary S, Prasad GN, Shenoi SD. Serpentine supravenous streaks induced by 5-fluorouracil. J Am Acad Dermatol 2005;53:529-30.
[Google Scholar]
|
| 4. |
Koehn GG, Balizet LB. Unusual local cutaneous reaction to dacarbazine. Arch Dermatol 1982;118:1018-9.
[Google Scholar]
|
| 5. |
Fine JD, Breathnach SM. Distinctive eruption characterized by linear supravenous papules and erythroderma following broxuridine (bromodeoxyuridine) therapy and radiotherapy. Arch Dermatol 1986;122:199-200.
[Google Scholar]
|
| 6. |
Geddes ER, Cohen PR. Antineoplastic agent-associated serpentine supravenous hyperpigmentation: Superficial venous system hyperpigmentation following intravenous chemotherapy. South Med J 2010;103:231-5.
[Google Scholar]
|
| 7. |
Chan CC, Lin SJ. Images in clinical medicine. Serpentine supravenous hyperpigmentation. N Engl J Med 2010;363:e8.
[Google Scholar]
|
Fulltext Views
4,801
PDF downloads
2,274





![[Figure - 1]](#fig_ijdvl_2015_81_4_434_156191_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2015_81_4_434_156191_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2015_81_4_434_156191_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2015_81_4_434_156191_f4.jpg){kind=link}