Translate this page into:
Serpiginous seborrhoeic keratosis: An unusual presentation following an eczematous dermatitis
2 Department of Pathology, Military Hospital, Ambala, India
Correspondence Address:
Ajay Kumar
Military Hospital, Ambala-133 001
India
| How to cite this article: Kumar A, Kashyap M, Pathania V. Serpiginous seborrhoeic keratosis: An unusual presentation following an eczematous dermatitis. Indian J Dermatol Venereol Leprol 2012;78:775-776 |
Sir,
Seborrhoeic keratoses (SK) are common benign nevoid epidermal tumors, frequently pigmented, with proliferation of basaloid and squamous keratinocytes and pseudo-horn cysts on histopathology. Though multiple lesions distributed in a linear or even a nevoid distribution may occur, a solitary lesion distributed in a serpiginous band has not been reported previously.
A 46-year old male presented with complaints of a dark patch on the back of 21 years duration. At the time of onset he had developed an itchy rash on the back with oozing. The dark patch appeared at the site of the rash and gradually increased in size and extent. A band like serpiginous dark pigmented plaque with a dull verrucous surface was observed on the right scapular region [Figure - 1]. The possibility of a verrucous epidermal naevus was considered. However, light microscopy examination of skin biopsy specimen revealed a papillomatous acanthotic epidermis with basaloid cells. A few horn cysts and pseudo-horn cysts were observed [Figure - 2]. On clinicopathological correlation, we arrived at a diagnosis of serpiginous SK.
 |
| Figure 1: Serpiginous band like dark pigmented plaque with a dull verrucous surface on the right scapular region |
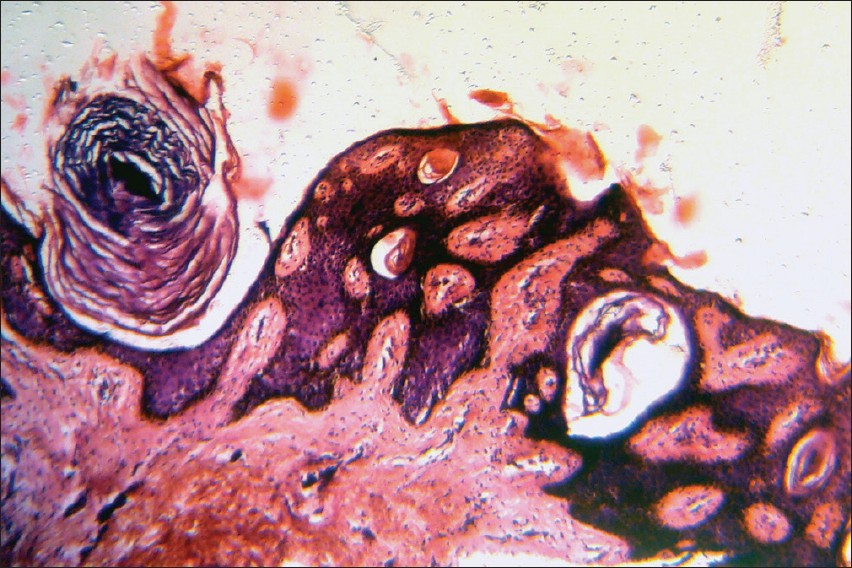 |
| Figure 2: Epidermis showing papillomatosis and acanthosis with proliferation of basaloid cells as well as horn cysts. A pseudo-horn cyst is opening to the surface (H and E, ×100) |
Gene expression of the tyrosinase kinase receptor, FGF receptor-3 and the transcription factor, forkland box N1 has been implicated in the formation of SK. The expression of these genes has been found to be enhanced in SK and suppressed in squamous cell carcinoma. [1]
SK may occur on any body site except the palms, soles or mucosae. Discrete dull, tan or brown papules or plaques with a verrucous surface and a ′stuck-on′ appearance may be aligned along skin folds. Nevoid distribution of lesions along Blaschko′s lines may occur. [2]
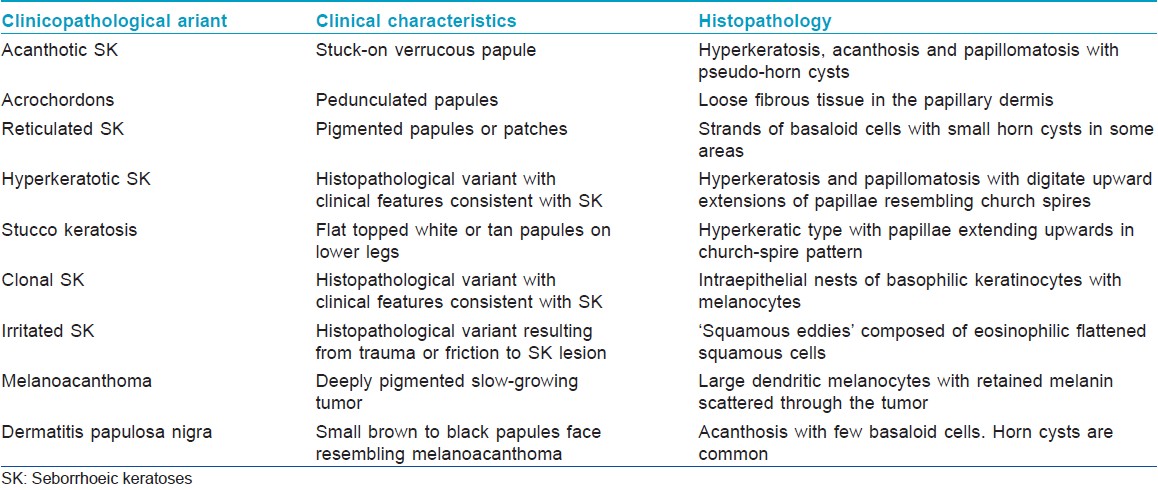
The histopathological features of SK are hyperkeratosis, acanthosis and papillomatosis with horny invaginations known as pseudo-horn cysts. [2] Proliferation of squamous cells and basaloid cells occurs in the acanthotic epidermis. Various clinical and histopathological variants of SK have been described [Table - 1].
The occurrence of eruptive SK after eczema was initially noted by Williams. [3] There are several reports of the development of SK following an inflammatory dermatosis such as erythrodermic eczema, [2] erythrodermic psoriasis and erythrodermic drug eruption [3] but mostly as eruptive SK. Elevated epidermal growth factor binding site activity correlates with actively growing SK. [4] An aberrant response to enhanced epidermal growth factor activity may explain eruptive SK after an inflammatory dermatosis.
The development of a solitary serpiginous SK lesion at the site of eczema in our patient however may be due to the isotopic phenomenon. Occurrence of an unrelated dermatological disease at the site of a healed disease is termed as isotopic phenomenon and cases have mostly occurred at the site of healed herpes zoster. [5] The cause of this phenomenon has been proposed to be locus minoris resistentiae or site of lowered resistance. Isotopic phenomenon occurring at the site of erstwhile eczematous dermatitis has not been reported.
| 1. |
Mandinova A, Kolev V, Neel V, Hu B, Stonely W, Lieb J, et al. A positive FGFR3/FOXN1 feedback loop underlies benign skin keratosis versus squamous cell carcinoma formation in humans. J Clin Invest 2009;119:3127-37.
[Google Scholar]
|
| 2. |
Thomas VD, Swanson NA, Lee KK. Benign epithelial tumors, hamartomas, and hyperplasias. In: Wolff K, Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, editors. Fitzpatrick's Dermatology in general medicine. 7 th ed. New York: McGraw Hill; 2007. p. 1054-67.
th ed. New York: McGraw Hill; 2007. p. 1054-67.'>[Google Scholar]
|
| 3. |
Flugman SL, McClain SA, Clark RA. Transient eruptive seborrheic keratosis associated with erythrodermic psoriasis and erythrodermic drug eruption: Report of two cases. J Am Acad Dermatol 2001;45:S212-4.
[Google Scholar]
|
| 4. |
Nanney LB, Ellis DL, Levine J, King LE. Epidermal growth factor receptors in idiopathic and virally induced skin diseases. Am J Pathol 1992;140:915-25.
[Google Scholar]
|
| 5. |
Madke B, Doshi B, Pande S, Khopkar U. Phenomena in dermatology. Indian J Dermatol Venereol Leprol 2011;77:264- 75.
[Google Scholar]
|
Fulltext Views
3,086
PDF downloads
2,392





![[Figure - 1]](#fig_ijdvl_2012_78_6_775_102400_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2012_78_6_775_102400_f2.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2012_78_6_775_102400_t3.jpg){kind=link}