Translate this page into:
Sign of Leser-Trélat in association with laryngeal carcinoma
Correspondence Address:
Asha Nyati
Government Medical College, Rangbadi Road, Kota - 324 009, Rajasthan
India
| How to cite this article: Nyati A, Kalwaniya S, Jain S, Soni B. Sign of Leser-Trélat in association with laryngeal carcinoma. Indian J Dermatol Venereol Leprol 2016;82:112 |
Sir,
The sign of Leser-Trélat, characterized by the sudden eruption of numerous seborrheic keratoses, often with associated pruritus, is considered a marker of internal malignancy.[1] Acanthosis nigricans may be associated with 20% of such cases.[1] The most frequently reported malignancies associated with the Leser-Trélat sign are stomach cancer, gastrointestinal adenocarcinoma and lymphoma.[2] Here, we report two cases of laryngeal carcinoma in siblings, both exhibiting the sign of Leser-Trélat.
The first patient was a known case of well-differentiated squamous cell carcinoma of larynx, detected 2 years previously on computed tomography (CT) neck, done as part of an evaluation for hoarseness of voice of recent onset. He received radiotherapy after which hoarseness resolved. Both post-therapy laryngoscopic examination and follow-up laryngoscopic examinations were normal till 1 month before presentation, when the hoarseness of voice recurred. This time, the patient noted the sudden appearance of multiple black-colored lesions over the trunk which were rapidly increasing in number and size prompting him to report to us. On examination, we found multiple seborrheic keratoses on his face, chest, abdomen and back [Figure - 1]a and [Figure - 1]b. The patient was not aware of the lesions on the back. The largest lesion was 1 × 1 cm in size and markedly darker than the usual seborrheic keratosis. Multiple cherry angiomas were also present, which were also very large and darker than usual. Otherwise, his general physical examination was normal. Laryngoscopic examination followed by computed tomography (CT) scan of the larynx confirmed recurrence of the tumor [Figure - 2]a,[Figure - 2]b,[Figure - 2]c. The complete blood counts, urea, electrolytes, liver function tests, chest radiograph, skeletal survey and ultrasonogram of the abdomen were normal. The skin lesions remained stable during chemoradiation.
 |
| Figure 1: Seborrheic keratoses arranged in “splash pattern” (a) on the patient's back and (b) anterior abdominal wall with a few large, dark cherry angiomas. (c) The patient's sister who also had laryngeal carcinoma showing seborrheic keratoses on both cheeks |
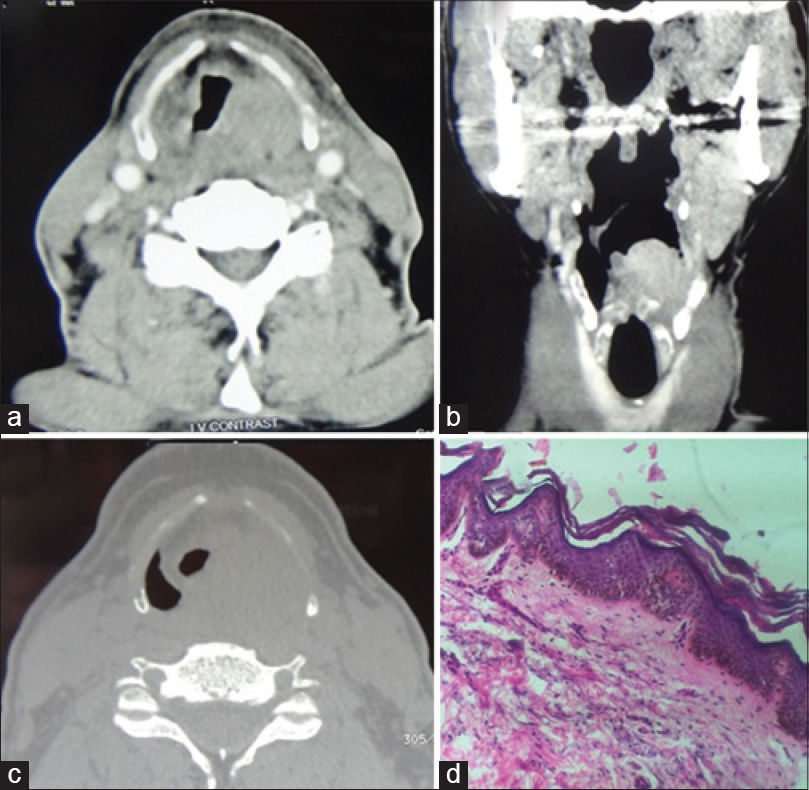 |
| Figure 2: Computed tomography, neck of the patient – (a) axial images in soft tissue window and (c) bone window along with (b) the corresponding coronal reformatted image shows soft tissue attenuation in the left supraglottic mass lesion without cartilage invasion or extra-laryngeal soft tissue component. (d) Pronounced papillomatosis, hyperkeratosis,mild acanthosis; verrucous appearance with elongated projections (”church spire” pattern) (H and E, ×100) seen in skin biopsy from the seborrheic keratoses lesion on back |
Interestingly, the patient's elder sister was also diagnosed with well-differentiated squamous cell carcinoma of the larynx on laryngoscopic biopsy of a right glottic growth, detected during evaluation of hoarseness of the voice. Meanwhile, she also started developing itchy eruptions of seborrheic keratoses on her face, [Figure - 1]c. Following radiotherapy of the laryngeal tumor, itching resolved but the seborrhoiec keratoses remained unchanged.
Leser-Trélat sign was originally described separately by Edmund Leser and Ulysse Trélat. It was first described together with eruptive cherry angiomas in patients having an internal malignancy. Later, Holländer described the relationship of seborrheic keratoses and cancer and the name of Leser-Trélat was given to this sign.[2] The sign of Leser-Trélat is characterized by the eruption of many new seborrheic keratoses, or a rapid increase in their size within weeks or months. This sign is described with stomach cancer, gastrointestinal adenocarcinoma, lymphoma, leukemia, mycosis fungoides, Sezary syndrome, breast carcinoma, lung carcinoma, prostate carcinoma and sarcomas (neurofibrosarcoma). The sign has also been reported in non-malignant situations as in heart transplant recipients, erythrodermic pityriasis rubra pilaris and human immunodeficiency virus infection.[2] The sign has even been described in a normal person.[1] We could find only a few previous reports of the Leser-Trélat sign in laryngeal carcinoma.[3]
The elderly have an increased incidence of both seborrheic keratoses and malignancy, so the validity of this entity as a paraneoplastic syndrome has been questioned.[2] However, there is an acute onset and rapid progression of seborrheic keratoses in the sign of Leser-Trélat, as was seen in our cases.[4] The criteria for Leser-Trélat sign defined by Ronchese are a rapid increase in seborrheic keratoses on lesion-free skin, pruritus and an accompanying internal malignancy. Heaphy et al. have suggested the term “Leser-Trélat syndrome” to describe the cases with accompanying internal malignancy.[2]
The pathomechanism of the sign of Leser-Trélat is unknown. The cause of the increase in size and number of seborrheic keratoses is thought to be an induction of epidermal proliferation by a growth factor secreted by the tumor cells.[1] It is believed that epidermal growth factor receptor (EGFR) overexpression may be one of the pathogenic mechanisms responsible for the sudden multiple eruption of seborrheic keratoses as immunohistochemical analyses of this protein has revealed an intense membranous staining in all epidermal layers, except the stratum corneum.[4]
Histopathology of the seborrhoiec keratoses in the sign of Leser-Trelat is similar to that of regular seborrheic keratoses [Figure - 2]d. There is no specific therapy, however, treatment of the associated neoplasm leads to regression of the seborrheic keratoses in approximately half the patients.[5]
| 1. |
Mittal RR, Sonal J. The sign of Leser-Trelat. Indian J Dermatol Venereol Leprol 2001;67:177.
[Google Scholar]
|
| 2. |
Turin E, Yesilova Y, Yurt N, Koçarslan S. Leser-Trélat sign: Does it really exist? Acta Dermatovenerol Croat 2013;21:123-7.
[Google Scholar]
|
| 3. |
Rubisz-Brzezinska J, Zebracka T, Musialowicz D. Coexistence of 2 paraneoplastic syndromes – Acrokeratosis bazex and Leser-Trèlat syndrome – In a case of squamous-cell laryngeal cancer. Przegl Dermatol 1983;70:205-8.
[Google Scholar]
|
| 4. |
Ponti G, Luppi G, Losi L, Giannetti A, Seidenari S. Leser-Trélat syndrome in patients affected by six multiple metachronous primitive cancers. J Hematol Oncol 2010;3:2.
[Google Scholar]
|
| 5. |
Ramos-E-Silva M, Carvalho JC, Carneiro SC. Cutaneous paraneoplasia. Clin Dermatol 2011;29:541-7.
[Google Scholar]
|
Fulltext Views
1,460
PDF downloads
1,200





![[Figure - 1]](#fig_ijdvl_2016_82_1_112_164222_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2016_82_1_112_164222_f2.jpg){kind=link}