Translate this page into:
Simultaneous occurrence of disseminated superficial, linear and hypertrophic verrucous forms of porokeratosis in a child
Correspondence Address:
Amiya Kumar Mukhopadhyay
�Pranab�, Ismile (Near Dharmaraj Mandir), Asansol, Dist. Burdwan, West Bengal - 713301
India
| How to cite this article: Mukhopadhyay A. Simultaneous occurrence of disseminated superficial, linear and hypertrophic verrucous forms of porokeratosis in a child. Indian J Dermatol Venereol Leprol 2004;70:364-366 |
Abstract
Porokeratosis is a genodermatosis characterized by abnormal epidermal keratinization with the histological feature of cornoid lamella. There are many clinical variants, but two or more of these variants rarely occur in a single patient. This variation in clinical presentation may be due to the different phenotypic expression of a common genetic abnormality or may be the consequence of abnormalities in closely linked genetic loci or genes. Here we report about a child who showed simultaneous occurrence of disseminated, linear and hypertrophic verrucous lesions of porokeratosis. He also had genital lesions, reported uncommonly in the medical literature.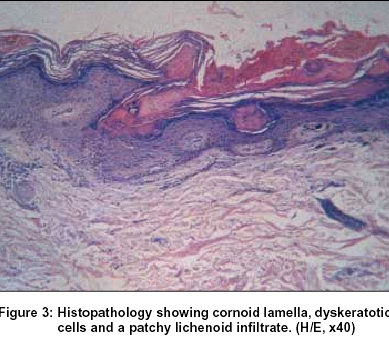 |
|
 |
|
 |
|
INTRODUCTION
Porokeratosis is a rare genodermatosis featuring abnormal epidermal keratinization, which is histologically characterized by the presence of cornoid lamella.[1] The term "porokeratosis" was first described by Vittorio Mibelli in 1893. Since then many variants of porokeratosis have been described, each with differing morphology, distribution and clinical course.[2] Classically five clinical variants are recognized: classic porokeratosis of Mibelli (CPM), disseminated superficial actinic porokeratosis (DSAP), disseminated superficial porokeratosis (DSP), porokeratosis palmaris et plantaris disseminata, and linear porokeratosis (LP).[3],[4] Apart from these five variants, a number of morphological forms, like facial porokeratosis, giant porokeratosis, punched out porokeratosis, hypertrophic verrucous porokeratosis (HVP), reticulate porokeratosis have been reported in the literature.[2] Coexistence of the different variants of porokeratosis in a single patient has been regarded as a rare occurrence.[1] Here we report a male child of 23 months of age who showed the simultaneous presence of DSP, LP and HVP, a combination yet undescribed in the literature.
CASE REPORT
A 23 month old male child was brought with pruritic multiple brownish to black, keratotic plaques on the left lower limb that began at the age of three months. Lesions subsequently developed on the right paranasal area, both ears, chest, left paravertebral region, left upper arm, knuckle of the right index finger, shaft of the penis and scrotum [Figure - 1]. The patient was otherwise healthy with no history of any major illness or drug therapy since birth. There was no incidence of similar disorder in his family.
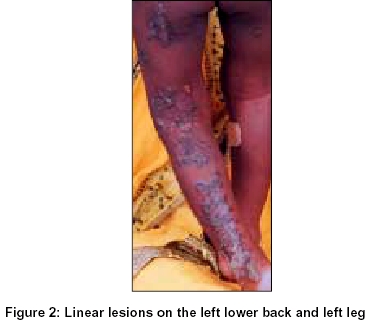
Examination showed widespread keratotic plaques. Lesions on posterior aspect of the left lower limb extending from lower back up to the heel, left lower chest, dorsum of the left foot and right knee were arranged in linear pattern. Other lesions were distributed over both exposed as well as covered areas of the body. He had no lesion on the palms, soles and mucosae. The lesions showed elevated borders, many of which revealed a thin groove on close inspection. Centres of many of the lesions were atrophic. A few lesions on the right knee were hyperkeratotic and verrucous in appearance [Figure - 2].
Histopathological examination of the tissue from the border of the lesion on the right lower limb showed the characteristic cornoid lamella and absent granular layer below the invagination. Upper dermis showed mild chronic inflammatory cell infiltration [Figure - 3]. The patient was treated with tretinoin cream (0.05%) twice daily and oral antihistaminic without much benefit.
DISCUSSION
The pathogenesis of porokeratosis is unknown. An autosomal mode of inheritance has been described,[4] but sporadic cases, as in the present patient may also occur. The presence of localized dysplastic features associated with the development of cornoid lamella suggests that the disease represents a focal, expanding clone of abnormal keratinocytes.[5] Although cornoid lamella may rarely be associated with some other conditions like viral warts, some ichthyoses and nevoid hyperkeratosis,[6] the clinical picture, etiology, and natural history of porokeratosis differentiates itself from these conditions. Porokeratosis has been shown to be associated with abnormal epidermal DNA ploides in association with increased DNA indices, midway between normal and Bowen′s disease.[7]
The similarities of clinical appearance and histopathology as well as the co-existence of different variants in one patient or in several members of an affected family indicates different phenotypic expressions of common genetic abnormality.[8] Alternately, genes of each subtype of porokeratosis may be carried on the same or closely linked loci, and thus coexistence of different subtypes could be explained based on simultaneous expression of closely linked genes.[1] A similar mechanism may be responsible in the present case.
Of the different subtypes, only CPM and LP are found commonly in childhood; DSAP remains clinically inapparent till adulthood and starts mostly in third and fourth decades.[3],[9] Although DSAP remains rare in children,[1] DSP manifests commonly between 5 and 10 years of age.[6] However, in our case DSP started in infancy. The linear variant of porokeratosis exists in two forms: in the more common localized form, lesions are unilateral, confined to one extremity and frequently distal in localization. In the rare generalized form, lesions are multiple, affect several extremities and involve the trunk.[10] Clinical features of the present case conform to the rare variety mentioned.
Though the lesions of porokeratosis may involve any part of the body, lesions on the genitalia are regarded as uncommon.[11] Our patient had lesions on both penis as well as scrotum representing this uncommon feature. Thus the coexistence of three different subtypes of porokeratosis along with the occurrence of DSP in infancy and affection of the genitalia in this patient prompted us to report this case.
| 1. |
Suh DH, Lee HS, Kim SD, Cho KH, Park KC. Coexistence of disseminated superficial porokeratosis in childhood with congenital linear porokeratosis. Pediatr Dermatol 2000;17:466-8.
[Google Scholar]
|
| 2. |
Rao MV, Singh A, Thappa DM, Ratnakar C. Hyperkeratotic verrucous porokeratosis. Indian J Dermatol 1998;43:120-1.
[Google Scholar]
|
| 3. |
Wollfe-Schreiner EC. Porokeratosis. In: Irwin FM, Eisen AZ, Wollf K, Austen KF, Goldsmith LA, Katz SI, et al, editors. Dermatology in General Medicine. 5th Ed. New York: McGraw Hill; 1999. p. 624-30.
[Google Scholar]
|
| 4. |
Lever WF, Lever SG. Histopathology of the skin. 7th Ed. Philadelphia: J B Lippincott Co; 1990. p. 70-2.
[Google Scholar]
|
| 5. |
Reed RJ, Leone P. Porokeratosis: A mutant clonal keratosis of the epidermis. I Histogenesis. Arch Dermatol 1970;101:340-7.
[Google Scholar]
|
| 6. |
Griffiths WA, Judge MR, Leigh IM. Disorder of keratinisation. In: Champion RH, Burton JI, Burns DA, Breathnach SM, editors. Rook/Wilkinson/Ebling Textbook of dermatology. 6th Ed. Oxford: Blackwell Science; 1998. p. 1552-4.
[Google Scholar]
|
| 7. |
McKee PH. Pathology of the skin with clinical correlations. 2nd Ed. London: Mosby-Wolfe; 1997. p. 221-53.
[Google Scholar]
|
| 8. |
Lucker GP, Steijlen PM. The coexistence of linear and giant porokeratosis with Bowen's disease. Dermatology 1994;189:78-80.
[Google Scholar]
|
| 9. |
Sigfried EC. The porokeratosis. In: Harper J, Orange A, Prose N, editors. Textbook of Pediatric Dermatology. Oxford: Blackwell Science; 2000. p. 1158-62.
[Google Scholar]
|
| 10. |
Laxmisha C, Thappa DM, Karthikeyan K, Jayanthi S. Linear porokeratosis along Blaschko's lines. Indian J Dermatol 2003;48:167-9.
[Google Scholar]
|
| 11. |
Neri I, Marzaduri S, Passarini B, Patrizi A. Genital porokeratosis of Mibelli. Genitourin Med 1995;71:410-1.
[Google Scholar]
|
Fulltext Views
2,309
PDF downloads
1,553





![[Figure - 1]](#fig_ijdvl_2004_70_6_364_13480_1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2004_70_6_364_13480_2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2004_70_6_364_13480_3.jpg){kind=link}