Translate this page into:
Skin complexion and pigmentary disorders in facial skin of 1204 women in 4 Indian cities
2 L'Or�al Research and Innovation, Bangalore, Karnataka, India
Correspondence Address:
Virginie Hourblin
Research Engineer, 2 Avenue Eug�ne Schueller, 93601 Aulnay-sous-bois
France
| How to cite this article: Hourblin V, Nouveau S, Roy N, de Lacharriere O. Skin complexion and pigmentary disorders in facial skin of 1204 women in 4 Indian cities. Indian J Dermatol Venereol Leprol 2014;80:395-401 |
Abstract
Background: The color of Indian skin shows great diversity and pigmentary disorders are a major concern of Indian women. Despite great variations in climate, diet, and social parameters within India, studies of the range of skin types have been rather scarce. Aims: This study was aimed at characterizing the color of Indian skin in various geographical locations, its characteristics in terms of overall skin complexion and pigmentary disorders, and the impact of age on these features. Methods: An extensive descriptive study, including skin color parameters (objective measurements and evaluations by dermatologists, clinically or from photographs) was carried out involving 1,204 female volunteers of different ages living in four different Indian cities. Results: Important differences in skin complexion according to the geographical location were observed. Age seemed to have little impact on complexion. Hyperpigmented spots were frequent and were noted at early stages and many lentigines were found. Melasma affected about 30% of middle-aged women, but many other ill defined, pigmented macules were also observed. Additionally, we found pigmented lip corners associated with marionette lines, and linear nasal pigmentation. Conclusions: Indian skin color is diverse and pigmentary disorders are common. Skin complexion is not greatly affected by age. Some hyperpigmented disorders occur at early stages and increase with age, contributing to overall unevenness of facial color.Introduction
Defining Indian skin as "Asian skin" or "skin of color" may lack accuracy, [1] although India clearly belongs to Asia geographically. The Indian population shows a remarkable diversity with more than 2,000 ethnic groups. In addition, great variations exist in terms of climate, diet, and social parameters within the country. In this context, Indian skin shows a wide variability in color as well as in some specific features. [2],[3],[4],[5] In particular, pigmentary disorders are a major concern in India and have a great psychosocial impact on quality of life. [6]
Surprisingly, there are few studies that have classified skin types in the Indian population. To fill such a gap, an extensive descriptive study based on a multifactorial evaluation approach, including some skin color parameters, was conducted on Indian women of different ages and from different cities. The main objective was to describe the characteristic features of facial skin color in Indian women in terms of overall skin complexion and pigmentary disorders, and to evaluate the impact of age upon these findings.
Skin color and pigmentary disorders assessments were performed using individual clinical examination by dermatologists, combined with visual evaluation on photographs and non-invasive colorimetric measurements.
METHODS
Subjects
We included 1204 women, aged 18-84 years from four Indian cities: Chennai, Mumbai, Kolkata, and Delhi. There were about 300 subjects per city with 25-28 women in each of 11 age groups: 18-24, 25-29, 30-34, 35-39, 40-44, 45-49, 50-54, 55-59, 60-64, 65-69, and over 70. Women were selected from the general population through print advertisements, without any restrictions of socio-economic status. We excluded women who were younger than 18 years, pregnant, having other illnesses which required care during the evaluation period and having illnesses with a high risk of transmission. Illiterate women were eligible for inclusion; in this case presence of a third party was required for reading and completing documents.
The study protocol was approved by the institutional review board in each city. All of the subjects provided signed informed consent prior to entering the study.
Dermatological assessments (clinical and on Visia® CR pictures)
All clinical assessments were performed by two dermatologists: one in Mumbai and the other in Chennai, Delhi, and Kolkata. To minimize a potential assessor effect, the same dermatologist from our group was present during study initiation in each city and trained both study dermatologists regarding the clinical gradations.
The dermatologists interviewed subjects for their medical history and clinically assessed facial skin complexion and pigmentary disorders (small hyperpigmented spots <3 mm, melasma, ill-defined patchily hyperpigmented macules, hypopigmentation, and hyperpigmented areas).
In addition, facial photographs of each subject were taken with Visia® CR booth (Canfield Scientific, Fairfield, USA). This system is used to capture standardized face pictures in different lighting conditions (standard, cross-polarized, parallel-polarized, and ultraviolet (UV)) and from three different angles (left, front, and right). All photographs were assessed by the dermatologist from our group.
Instrumental measurements (Chroma Meter® )
Skin color measurements were performed on the photo-exposed skin of the cheek and on the photoprotected skin of the upper inner arm as reference, using the Chroma Meter® CR-400 (Konica Minolta, Tokyo, Japan). This device measures the intensity of reflected light and the color of the skin surface. The skin surface is illuminated with polychromatic light and the signal from the skin is reflected into the device and separated into its spectral components using the LFNx01aFNx01bFNx01 system of the ("Commission Internationale de l′Eclairage" (CIELab). Briefly, the components are LFNx01 for luminance/brightness (the higher the value, the higher the intensity), aFNx01 for red/green components of light, positive values representing the red component and negative values representing the green component, and bFNx01 for yellow/blue components of light, positive values representing the yellow component of the light and negative values representing the blue component.
All measurements were performed by the same technician in each city and repeated three times per area.
Statistical analysis
Data collection and data management were carried out for each of the cities using an electronic case report form (eCRF) that complied with Good Clinical Practices.
Statistical Analysis System (SAS)® 9.3 statistical software was used to perform descriptive analyses (graphics and tables) for all descriptors. Analyses were displayed by age and city. Probability of P < 0.05 was used as the threshold for significance. Analysis of variance was performed to compare evaluations across cities.
RESULTS
Skin complexion
Clinical assessment revealed several grades of skin complexion among the Indian women included in this study [Figure - 1]. The clinical assessment correlated with Chroma Meter® measurements of brightness (LFNx01), which decreases when skin complexion becomes darker.
The distribution of skin complexions was different in the women included at the 4 study locations [Figure - 2]a and b.
 |
| Figure 1: Skin complexion: dermatologist assessment |
 |
| Figure 2 |
In the Mumbai group, the lightest skin complexions "wheatish" and "medium brown" were the most prevalent (N = 135 (45%) and N = 103 (34%), respectively). In the Delhi group, "brown" and "medium brown" were the most prevalent skin complexions (N = 118 (41%) and N = 97 (34%), respectively), In the Kolkata group, "brown" and "medium brown" were the most prevalent skin complexions (N = 115 (37%) and N = 121 (39%), respectively) while in the Chennai group, the darkest skin complexions "brown" and "dark brown" were the most prevalent (N = 117 (38%) and N = 110 (36%), respectively). The mean brightness (LFNx01) value of Chroma Meter® measurements in the Chennai study location was significantly lower than in the other cities (P < 0.0001).
The skin color overall did not change much with age. Skin darkening with age was found in the Chennai study location (a decrease of brightness LFNx01 by 12%, P < 0.0001), but was mild; it was not observed in the other study locations [Figure - 3]a. Between 18 and 35 years, there was a very low decrease in brightness (LFNx01) on both photo-exposed and photo-protected skin. [Figure - 3]b. After 35 years, the skin became a bit fairer with age on photo-protected areas (brightness LFNx01 increased by 6%), while it became barely darker on photo-exposed areas (brightness LFNx01decreased by 2%).
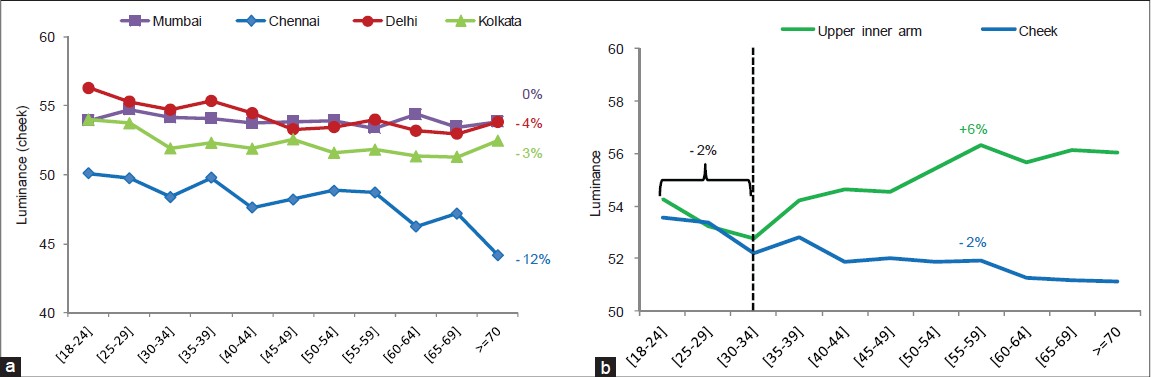 |
| Figure 3: (a) Average skin luminance according to age group in Mumbai, Chennai, Delhi, and Kolkata— measured on the cheek with Chroma Meter® (N = 1,202). (b) Average skin luminance in age groups measured on cheek (photo-exposed area) and upper inner arm (photoprotected area) (N = 1,202) |
Pigmentary disorders
Hyperpigmented spots
0Descriptive analyses of the following pigmentary disorders did not reveal any obvious differences in the different study locations.
Clinical assessment revealed hyperpigmented spots on the face in all women [Figure - 4]. The proportion of women who had more than 10 hyperpigmented spots on the face was more than 70% (N = 708/986) in women over 30 years of age [Figure - 5]a. Before the age of 40 years, most of these small spots were post-inflammatory marks due to acne. After the age of 30 years, lentigines were noted in 860 (87%) women but it was difficult to differentiate simple lentigines from actinic lentigines. Many seborrheic keratosis were also observed in 688 (70%) women.
 |
| Figure 4: Hyperpigmented spots |
 |
| Figure 5: (a) Prevalence of hyperpigmented spots (according to age group) assessed clinically by dermatologists (N = 1,204). (b) Prevalence of hyperpigmented spots (according to age group) assessed from photographs (N = 1,196) |
Assessments of photographs confirmed that almost all women had hyperpigmented spots on the forehead, malar, and mandibular areas [Figure - 5]b. The malar area was most commonly involved with 695 (80%) women over 35 years having moderate to severe spots.
Melasma and ill-defined patchy pigmented macules
Clinical assessment revealed melasma in many women [Figure - 6] with a peak prevalence of about 30% (N = 147/547) in women aged from 40 to 65 years [Figure - 7]. The mean age of women with melasma was 51 years. The findings on clinical assessment were confirmed on reviewing photographs of subjects.
 |
| Figure 6: Melasma and patchy pigmented macules |
 |
| Figure 7: Prevalence of melasma (according to age group) assessed clinically by dermatologists (N = 1,204) |
The prevalence of melasma in the Mumbai study location was 27.7% (N = 83), compared to the other locations where the prevalence was 15.3% (N = 47) in the Chennai group, 17.1% (N = 49) in the Delhi group and 15.6% (N = 48) in the Kolkata group. This difference was statistically significant (P < 0.0001).
Evaluation of photographs revealed the presence of another kind of hyperpigmentation on the face: ill-defined pigmented macules. These lesions were larger than hyperpigmented spots, poorly marginated and show variegated pigmentation. They differed from melasma which is usually symmetrical. The prevalence of such moderate to markedly pigmented macules increased with age, particularly on the malar area [Figure - 8] in up to 70% of women (P < 0.0001).
 |
| Figure 8: Prevalence of pigmented macules on forehead, malar, or mandible area (according to age group) assessed from photographs (N = 1,196) |
Hypopigmented spots or areas
117 women (less than 10%) showed disorders of hypopigmentation. The main conditions noted were post-inflammatory hypopigmented macules and pityriasis alba [Table - 1]. Only 11 (1%) subjects had vitiligo. The prevalence of hypopigmented lesions varied from 5.2% (N = 16) in the Chennai group to 15.0% (N = 45) in the Mumbai group (P < 0.0001).

Hyperpigmented areas
Clinical assessment revealed that almost all women had dark circles on the upper and lower eyelids, with intensity increasing with age [Figure - 9]a. The proportion of women with moderate to severe dark circles on the upper eyelid increased with age from 50% (N = 52/108) to 85% (N = 94/111) [Figure - 10]. Photographic evaluation confirmed that 1085 (91%) women had darker periorbital areas.
 |
| Figure 9: Specific hyperpigmented areas: (a) Periorbital area, (b) lip corners, and (c) nose bridge |
 |
| Figure 10: Prevalence of moderately to severely hyperpigmented areas (according to age group) assessed clinically by dermatologists (N = 1,204) |
Perilabial pigmentation was very frequent: 356 (30%) women showed moderate to severe pigmentation of the upper lip. Clinical assessment revealed that 705 (72%) women over 30 years had moderate to severe pigmentation of the corners of the lips [Figure - 9]b and [Figure - 10]. Three hundred and seventy three (38%) women over 30 years showed moderately to severely pigmented marionette lines.
A distinctive finding was pigmentation of the nose . Five hundred and fifty four (46%) women showed pigmentation at the angles of the nose. In addition, 296 (25%) women had a hyperpigmented line across the nose (42% of Mumbai women); in some of them the line was broad and divided the nose into a darker area on top and a lighter area below [Figure - 9]c and [Figure - 10]. The prevalence of this disorder increased with age from 10 to 30%.
DISCUSSION
In the present study, conducted in four Indian cities, a range of skin complexions were represented, from light to dark. The relative proportions of different complexions differed between study sites with darker complexions seen more frequently in subjects at the Chennai study location.
We found that aging did not significantly affect complexion which barely darkened with age. Skin darkening with age has previously been described in various populations, for example, a Chinese group living in Chicago as reported by de Rigal et al., [7] However, such age-related changes were not observed in African-Americans, Caucasians, and Mexicans. A recent study on Chinese women living in China [8] showed progressive darkening of the complexion with advancing age. A more recent study conducted in eight Asian cities found that Asian skin is generally darker with age. [9]
Using colorimetry to objectively record changes, we found that after 35 years of age, there was a slight whitening of unexposed skin and a slight darkening on the exposed area with age. This may account for the overall impression of facial darkening compared to the whole body, even though darkening is mild. Similar studies have been reported in other ethnic groups. In a cohort of 653 Caucasians, a significant darkening of exposed areas was observed after 20 years. However, amongst 497 Koreans, skin color remained rather stable with age, as in our subjects. [10],[11]
Our data confirmed the importance of pigmentary disorders in the Indian general population, particularly a significant prevalence of small hyperpigmented spots irrespective of age. Some disorders have already been described in India: [12] hypopigmentation, such as vitiligo, pityriasis alba, or versicolor; and also hyperpigmentation, such as melasma and some other facial melanoses. [13],[14],[15],[16] A few studies document the increased frequency of disorders characterized by hyperpigmentation in darker ethnic groups. [17],[18],[19],[20]
Hypopigmented disorders such as pityriasis alba (2.3%) and vitiligo (0.9%) were seen infrequently in our study. A slightly higher prevalence of pityriasis alba (3.6%) was reported in a survey of 1275 subjects in mountainous north India. [21] The prevalence of vitiligo ranges between 0.5 and 2% in the general population worldwide, which appears consistent with our results. [22]
Surprisingly, many lentigo simplex were noted during clinical assessment. This high prevalence, and the early onset of actinic lentigines and seborrheic keratosis (around 30 years) [23] does not appear to have been described previously. Histopathological analyses need to be carried out to better understand these disorders.
According to our data, melasma affects one-third of women between 40 and 65 years, an overall prevalence consistent with that found in other countries. [24],[25] In addition, we noted ill-defined, patchily hyperpigmented macules which caused greater concern to our subjects than melasma. These pigmented macules steadily increased with age, unlike the bell curve distribution of melasma prevalence along life span.
Some facial areas showed homogeneous hyperpigmentation, in particular periorbital, perilabial, and nose areas. More than 50% of women were concerned by such pigmentation, increasing up to 80% after the age of 35 years. Periorbital melanosis is well-known and described in Indian skin. [13] In addition, we found 2 other characteristic pigmentary findings in our subjects, both of which caused major concern: pigmentation of the lip corners associated with pigmented marionette lines, noted in 70% of subjects and pigmentation of the nose, noted in 50%. Recent studies have described linear pigmentation across the nose associated with a groove or ridge, referred to as transverse nasal groove or nasal crease. The crease has been particularly emphasized in the case of the allergic salute. [26],[27] Our study did not evaluate any changes in the contour of the skin and we noted only the linear nasal pigmentation. The self-perception of uneven skin color is contributed to by these various pigmentary changes.
To our knowledge, this is the first descriptive study of the complexion of Indian skin in the general population; most previous reports included only people consulting in dermatological centers. A sample size of 1,200 women may appear small considering the immense size of the Indian population but it is large enough to permit statistical analysis. In addition, we followed a rigorous study protocol composed of individual clinical examinations by dermatologists and objective colorimetric measurements.
Our study confirmed the diversity of Indian skin color as well as the importance of pigmentary disorders. Interestingly, we found that overall facial skin complexion is not greatly affected by age but that hyperpigmented disorders appear early in life and increase with age contributing to an overall unevenness of facial pigmentation. There is a need to further characterize and explore the mechanisms underlying the early onset and high prevalence of hyperpigmented spots, ill defined, patchy pigmented macules, and specific pigmented lines observed in this population.
Acknowledgment
We thank all the L′Oréal collaborators involved in this project, in particular Loïc Colomb, Olivier Coubard, Surekha Shetti, Tomoo Hanaya, Daniel Ye, Philippe Bastien, and Claire Battie for their important contribution and support.
| 1. |
Verma SB. Redefining color of Indian skin. J Eur Acad Dermatol Venereol 2008;22:1263-4.
[Google Scholar]
|
| 2. |
Jaswal IJ. Pigmentary variation in Indian populations. Acta Anthropogenet 1983;7:75-83.
[Google Scholar]
|
| 3. |
Jaswal IJ. Skin color in north indian populations. J Hum Evol 1979;8:361-6.
[Google Scholar]
|
| 4. |
Verma SB. Dermatology for the elderly: An Indian perspective. Clin Dermatol 2011;29:91-6.
[Google Scholar]
|
| 5. |
Reich D, Thangaraj K, Patterson N, Price AL, Singh L. Reconstructing Indian population history. Nature 2009;461:489-94.
[Google Scholar]
|
| 6. |
Shenoi SD, Prabhu S. Role of cultural factors in the biopsychosocial model of psychosomatic skin diseases: An Indian perspective. Clin Dermatol 2013;31:62-5.
[Google Scholar]
|
| 7. |
de Rigal J, Des Mazis I, Diridollou S, Querleux B, Yang G, Leroy F, et al. The effect of age on skin color and color heterogeneity in four ethnic groups. Skin Res Technol 2010;16:168-78.
[Google Scholar]
|
| 8. |
Huixia Q, Xiaohui L, Chengda Y, Yanlu Z, Senee J, Laurent A, et al. Instrumental and clinical studies of the facial skin tone and pigmentation of Shanghaiese women. Changes induced by age and a cosmetic whitening product. Int J Cosmet Sci 2012;34:49-54.
[Google Scholar]
|
| 9. |
Galzote C, Estanislao R, Suero MO, Khaiat A, Mangubat MI, Moideen R, et al. Characterization of facial skin of various Asian populations through visual and non-invasive instrumental evaluations: Influence of age and skincare habits. Skin Res Technol 2013;19:454-65.
[Google Scholar]
|
| 10. |
Lock-Anderson J, Knudstorp ND, Wulf HC. Facultative skin pigmentation in caucasians: An objective biological indicator of lifetime exposure to ultraviolet radiation? Br J Dermatol 1998;138:826-32.
[Google Scholar]
|
| 11. |
Roh K, Kim D, Ha S, Ro Y, Kim J, Lee H. Pigmentation in Koreans: Study of the differences from Caucasians in age, gender and seasonal variations. Br J Dermatol 2001;144:94-9.
[Google Scholar]
|
| 12. |
Pasricha JS, Khaitan BK, Dash S. Pigmentary disorders in India. Dermatol Clin 2007;25:343-52.
[Google Scholar]
|
| 13. |
Khanna N, Rasool S. Facial melanoses: Indian perspective. Indian J Dermatol Venereol Leprol 2011;77:552-63.
[Google Scholar]
|
| 14. |
Sarkar R, Puri P, Jain RK, Singh A, Desai A. Melasma in men: A clinical, aetiological and histological study. J Eur Acad Dermatol Venereol 2010;24:768-72.
[Google Scholar]
|
| 15. |
Somani VK, Razvi F, Sita VN. Pigmentary demarcation lines over the face. Indian J Dermatol Venereol Leprol 2004;70:336-41.
[Google Scholar]
|
| 16. |
Malakar S, Lahiri K, Banerjee U, Mondal S, Sarangi S. Periorbital melanosis is an extension of pigmentary demarcation line-F on face. Indian J Dermatol Venereol Leprol 2007;73:323-5.
[Google Scholar]
|
| 17. |
Halder RM, Grimes PE, McLaurin CI, Kress MA, Kenney JA Jr. Incidence of common dermatoses in a predominantly black dermatologic practice. Cutis 1983;32:388, 390.
[Google Scholar]
|
| 18. |
Sanchez MR. Cutaneous diseases in Latinos. Dermatol Clin 2003;21:689-97.
[Google Scholar]
|
| 19. |
Alexis AF, Sergay AB, Taylor SC. Common dermatologic disorders of skin of color: A comparative practice survey. Cutis 2007;80:387-94.
[Google Scholar]
|
| 20. |
Grimes PE. Management of hyperpigmentation in darker racial ethnic groups. Semin Cutan Med Surg 2009;28:77-85.
[Google Scholar]
|
| 21. |
Grills N, Grills C, Spelman T, Stoove M, Hellard M, El-Hayek C, et al. Prevalence survey of dermatological conditions in mountainous north India. Int J Dermatol 2012;51:579-87.
[Google Scholar]
|
| 22. |
Krüger C, Schallreuter KU. A review of the worldwide prevalence of vitiligo in children/adolescents and adults. Int J Dermatol 2012;51:1206-12.
[Google Scholar]
|
| 23. |
Hölzle E. Pigmented lesions as a sign of photodamage. Br J Dermatol 1992;127:48-50.
[Google Scholar]
|
| 24. |
Werlinger KD, Guevara IL, Gonzalez CM, Rincon ET, Caetano R, Haley RW, et al. Prevalence of self-diagnosed melasma among premenopausal Latino women in Dallas and Fort Worth, Tex. Arch Dermatol 2007;143:424-5.
[Google Scholar]
|
| 25. |
Sivayathorn A. Melasma in orientals. Clin Drug Invest 1995;10:24-40.
[Google Scholar]
|
| 26. |
Sathyanarayana BD, Basavaraj HB, Nischal KC, Swaroop MR, Umashankar PN, Agrawal DP, et al. Appraisal of transverse nasal groove: A study. Indian J Dermatol Venereol Leprol 2012;78:439-42.
[Google Scholar]
|
| 27. |
Myers WA, The "nasal crease". A physical sign of allergic rhinitis. JAMA 1960;174:1204-6.
[Google Scholar]
|
Fulltext Views
13,601
PDF downloads
3,899





![[Figure - 1]](#fig_ijdvl_2014_80_5_395_140290_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2014_80_5_395_140290_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2014_80_5_395_140290_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2014_80_5_395_140290_f4.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2014_80_5_395_140290_f5.jpg){kind=link}
![[Figure - 6]](#fig_ijdvl_2014_80_5_395_140290_f6.jpg){kind=link}
![[Figure - 7]](#fig_ijdvl_2014_80_5_395_140290_f7.jpg){kind=link}
![[Figure - 8]](#fig_ijdvl_2014_80_5_395_140290_f8.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2014_80_5_395_140290_t11.jpg){kind=link}
![[Figure - 9]](#fig_ijdvl_2014_80_5_395_140290_f9.jpg){kind=link}
![[Figure - 10]](#fig_ijdvl_2014_80_5_395_140290_f10.jpg){kind=link}