Translate this page into:
Solitary dome-shaped erythematous lump of long duration on the palm
2 Department of Pathology, University College of Medical Sciences and GTB Hospital, University of Delhi, New Delhi, India
Correspondence Address:
Deepika Pandhi
Department of Dermatology and STD, University College of Medical Sciences and GTB Hospital, University of Delhi, New Delhi - 110 095
India
| How to cite this article: Daulatabad D, Pandhi D, Tanveer N, Sharma S, Kaur I. Solitary dome-shaped erythematous lump of long duration on the palm. Indian J Dermatol Venereol Leprol 2018;84:437-439 |
Clinical Case
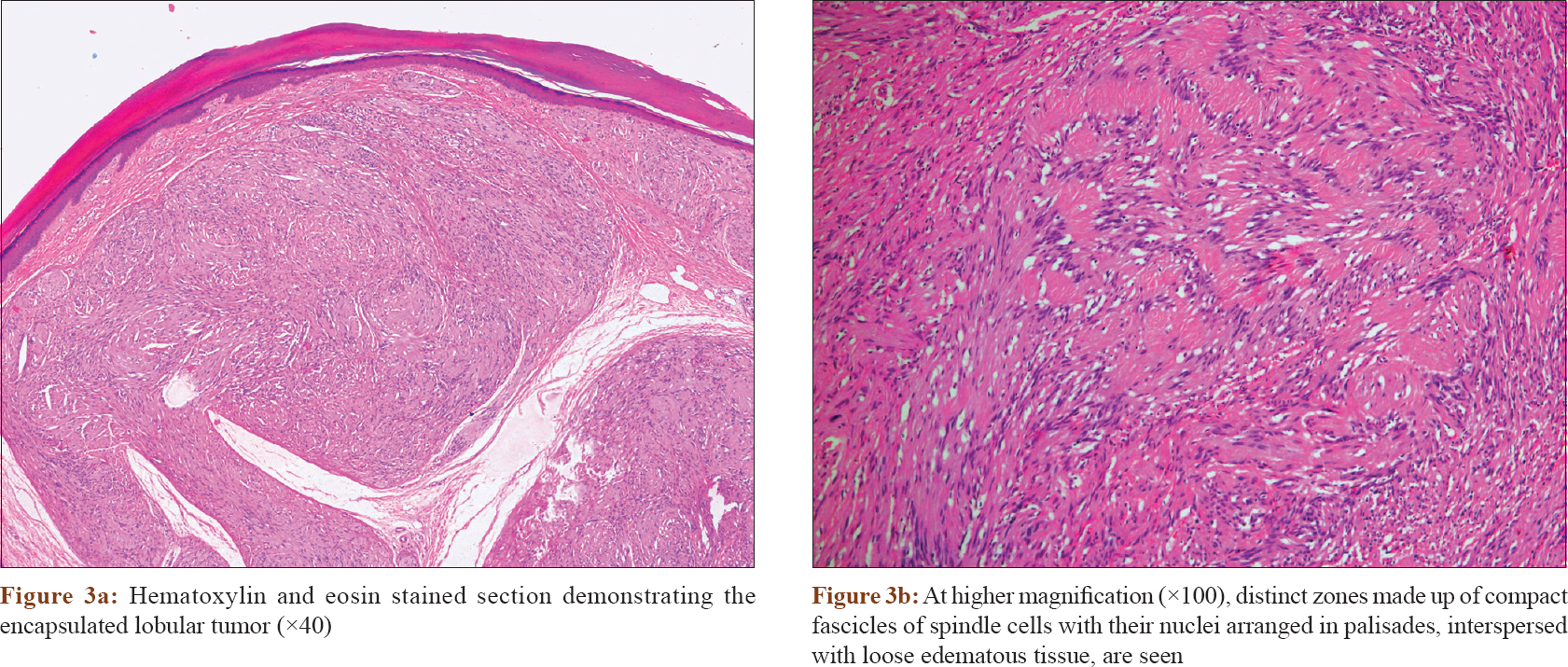
An 18-year-old girl presented to us with a solitary dome-shaped erythematous nodule on her right palm present since 10 years of age [Figure - 1]. The lump was asymptomatic, gradually progressive with no preceding history of trauma or evidence of neurological deficit. Dermoscopy revealed a multi-lobulated lesion with multiple arborizing vessels of varying caliber and speckled pigmentation overlying a translucent yellowish background [Figure - 2]. General examination and medical history were unremarkable. Excisional biopsy and histopathological examination (hematoxylin and eosin stain) revealed an encapsulated lobular tumor abutting the dermis with thinning of the overlying epidermis.[Figure - 3]a. At higher magnification (×100) we observed distinct zones made up of compact fascicles of spindle cells with their nuclei arranged in palisades interspersed with loose edematous tissue.[Figure - 3]b.
 |
| Figure 1: Single erythematous nodule on the right palm |
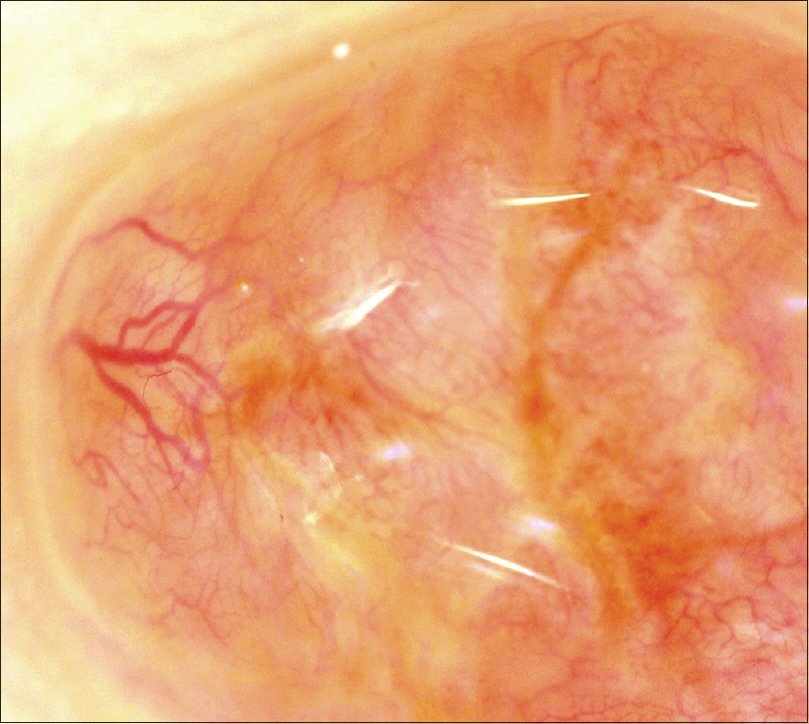 |
| Figure 2: Lobulated structure with multiple small and large caliber arborizing vessels. Pink-yellow structureless areas and speckled brown pigmentation, with highest density along the septa separating the lobules (×50, Dino-lite pro-polariser USB dermoscope, under oil) |
 |
What Is Your Diagnosis?
Answer
Diagnosis: Cutaneous schwannoma.
Discussion
Schwannoma is one of the peripheral nerve sheath tumors derived from the Schwann cells, which are responsible for the production of myelin sheath surrounding the peripheral nerves. As these cells are also called neurilemmocytes, the tumor is also known as neurilemmoma. These often present as swellings along the large peripheral or cranial nerves, the most common being acoustic neuroma.
The peak incidence is seen in the fourth to fifth decade of life with no sexual predilection. When involving the skin, these lesions are known as cutaneous schwannomas which usually present as ill-defined soft tissue swellings or lumps due to their deep subcutaneous location. These are usually asymptomatic but may present with pain or local sensory impairment or paresthesias in one-third of the cases. These are slow growing, encapsulated tumors that follow a benign course and rarely undergo malignant transformation. The most common presentation is that of a solitary tumor, but multiple lesions may also be seen, which mandate evaluation for underlying neurofibromatosis type I and schwannomatosis.
Cutaneous schwannomas are often diagnosed after surgical excision based on their classical histopathology, The tumor is encapsulated by perineurium and characterized by two distinct histological patterns: Antoni type A and Antoni type B depicted distinctly in [Figure - 4]. The former is a highly ordered cellular pattern with spindle cells arranged in compact fascicles with their nuclei arranged in palisades. Verocay bodies are formed by the acellular processes that separate adjacent rows of palisaded nuclei within the Antoni type A tissue. Antoni type B tissue is less cellular with pale zones of gelatinous matrix and evidence of cystic, edematous or myxoid degeneration.[1] Clinically, palisaded encapsulated neuroma (PEN) also presents as a solitary flesh colored dome-shaped tumor but can be differentiated histologically. It is a partially encapsulated mass of interweaving fascicles of spindle cells separated by small clefts, located in the papillary dermis. Immunohistochemistry of schwannoma, as well as PEN, reveals positivity for S100 and collagen type IV, while the capsule stains for epithelial membrane antigen. Another close differential of schwannomas is malignant peripheral nerve sheath tumors. Apart from having fascicles of alternating cellularity and palisades as in schwannoma, malignant peripheral nerve sheath tumor may also have whorls or rosette-like arrangements, perineural/intraneural spread when associated with nerve, subendothelial accentuation of tumor cells and large areas of necrosis in a geographic pattern. Cellular nuclear atypia, mitotic figures and bizzare cells may also be seen. None of these features were observed in our case which helped us differentiate between the two.
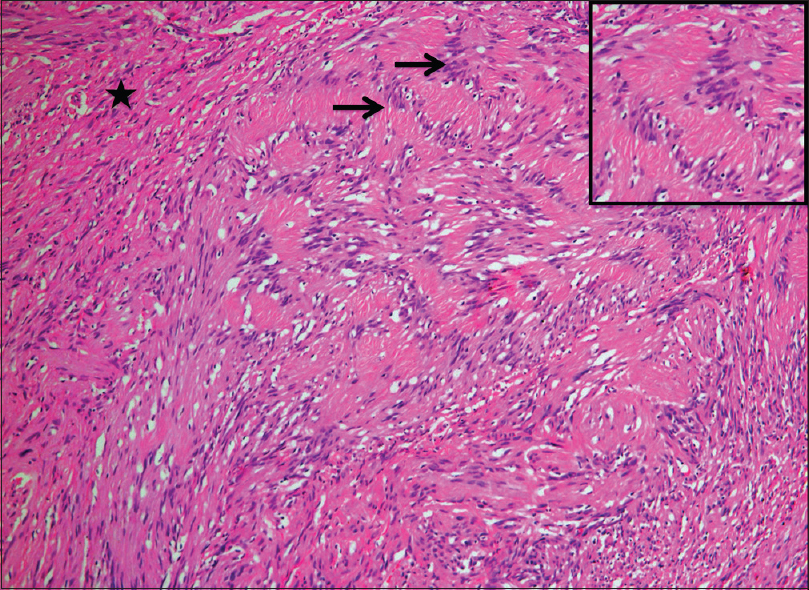 |
| Figure 4: The classical Antoni type A tissue is depicted with arrow and Antoni type B with star (×100, H and E). The inset shows a well formed Verocay body. |
In our case a very superficial localization of the tumor was observed and differentials such as eccrine poroma, nodular basal cell carcinoma and amelanotic melanoma were considered. Since such superficial lesions of schwannoma are a rarity with scarce reports so far, dermoscopic features of the tumour have not yet been reported.[2],[3],[4] However, the absence of classical dermoscopic features of eccrine poroma such as irregular linear and branched vessels with semi-elliptical or semicircular endings (“chalice-form” and “cherry-blossoms” vessels) or structure-less pink-white areas [5] and the absence of halo around the vessels [6] raised our index of suspicion.
Apart from arborizing vessels and speckled pigmentation, no other characteristic dermoscopic feature of nodular basal cell carcinoma-was observed like leaf-like pattern or blue nests. Histology clinched the final diagnosis in our case.
The treatment involves complete excision while avoiding damage to the nerve of origin. Hence, it is prudent to consider schwannoma in such cases and perform a histopathological examination to circumvent risk of incomplete removal or damage to the parent nerve.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Kurtkaya-Yapicier O, Scheithauer B, Woodruff JM. The pathobiologic spectrum of schwannomas. Histol Histopathol 2003;18:925-34.
[Google Scholar]
|
| 2. |
Cho SB, Kim HS, Paik JH, Ryu DJ, Oh SH. Dome-shaped tumour with surface changes on the abdominal wall. Clin Exp Dermatol 2010;35:95-6.
[Google Scholar]
|
| 3. |
Choi YS, Shin MS, Park MY, Park HJ. Case of cystic schwannoma. J Dermatol 2008;35:751-3.
[Google Scholar]
|
| 4. |
Noh S, Do JE, Park JM, Jee H, Oh SH. Cutaneous schwannoma presented as a pedunculated protruding mass. Ann Dermatol 2011;23 Suppl 2:S264-6.
[Google Scholar]
|
| 5. |
Espinosa AE, Ortega BC, Venegas RQ, Ramírez RG. Dermoscopy of non-pigmented eccrine poromas: Study of Mexican cases. Dermatol Pract Concept 2013;3:25-8.
[Google Scholar]
|
| 6. |
Ferrari A, Buccini P, Silipo V, De Simone P, Mariani G, Marenda S, et al. Eccrine poroma: A clinical-dermoscopic study of seven cases. Acta Derm Venereol 2009;89:160-4.
[Google Scholar]
|
Fulltext Views
4,300
PDF downloads
2,903





![[Figure - 1]](#fig_ijdvl_2018_84_4_437_224223_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2018_84_4_437_224223_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2018_84_4_437_224223_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2018_84_4_437_224223_f4.jpg){kind=link}