
Translate this page into:
Spontaneous regression of aggressive cutaneous squamous cell carcinoma
Corresponding author: Dr. Magí Brufau-Cochs, Department of Dermatology, Hospital Clínic de Barcelona, C. de Villarroel, Barcelona, Spain. mbrufaucochs@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Brufau-Cochs M, Sandoval-Clavijo A, García-Herrera A, Toll-Abelló A. Spontaneous regression of aggressive cutaneous squamous cell carcinoma. Indian J Dermatol Venereol Leprol. 2025;91:386-8. doi: 10.25259/IJDVL_1205_2023
Keywords
Spontaneous regression
cutaneous squamous cell carcinoma
immunotherapy
cemiplimab

Dear Editor,
Surgical management of cutaneous squamous cell carcinoma (CSCC) is the most common approach in the early stages, although systemic treatments might be necessary in advanced stages.1 We here describe a patient who presented with complete spontaneous regression of a CSCC with loco-regional dissemination, a situation only reported once before.2
A male patient in his 90s presented with a 3-month history of an asymptomatic, rapidly growing lesion on the left parietal area within a large cancerisation field. Physical examination revealed a 10 cm × 13 cm flesh-coloured tumour with satellite lesions compatible with in-transit metastases in the left temporal region as well as indurated nodules in the lateral cervical area [Figure 1]. Head and neck magnetic resonance imaging showed non-specific multiple left-cervical lymph nodes less than 1 cm in diameter. He had a previous history of an atypical fibroxanthoma in the left parieto-occipital area that had been removed 3 years before. In addition, the patient also had a documented 6-year history of an asymptomatic and stable renal mass with a radiological appearance of a clear cell carcinoma. The patient refused both treatment and invasive diagnostic procedures for this condition. Consequently, such tumour was only controlled with clinical and radiological assessments which demonstrated no progression or evidence of disseminated disease [Figure 2].

- Clinical image of the squamous cell carcinoma and its satellite lesions on the temporal zone. The black arrow indicates the satellite lesion selected for biopsy.
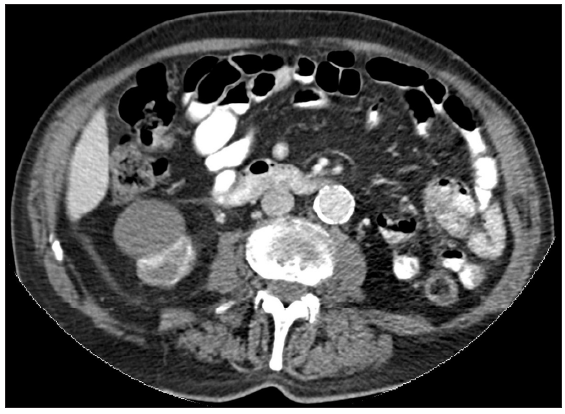
- Computed tomography scan documenting the right renal mass.
A punch biopsy from a satellite lesion of the temporal zone [Figure 1] was compatible with the diagnosis of an in-transit metastasis of a well-differentiated CSCC [Figure 3a, 3b and, 3c]. The tumour was staged as T3,Nx,M0 by the American Joint Committee on Cancer 8th edition. Cemiplimab was prescribed for treatment when the tumour was deemed inoperable. Approval for treatment was obtained after two months. However, upon the scheduled commencement date for Cemiplimab, a noticeable improvement was observed, with the cutaneous tumour showing signs of flattening. Over the following 12 weeks, progressive amelioration and complete resolution of the lesion were observed without any treatment being started [Figure 4]. Furthermore, a control computed tomography scan showed no abnormal lymph nodes. A new 2 cm non-metastatic CSCC tumour appeared 22 months after the resolution of the lesion and was treated with radiotherapy with no further relapses.
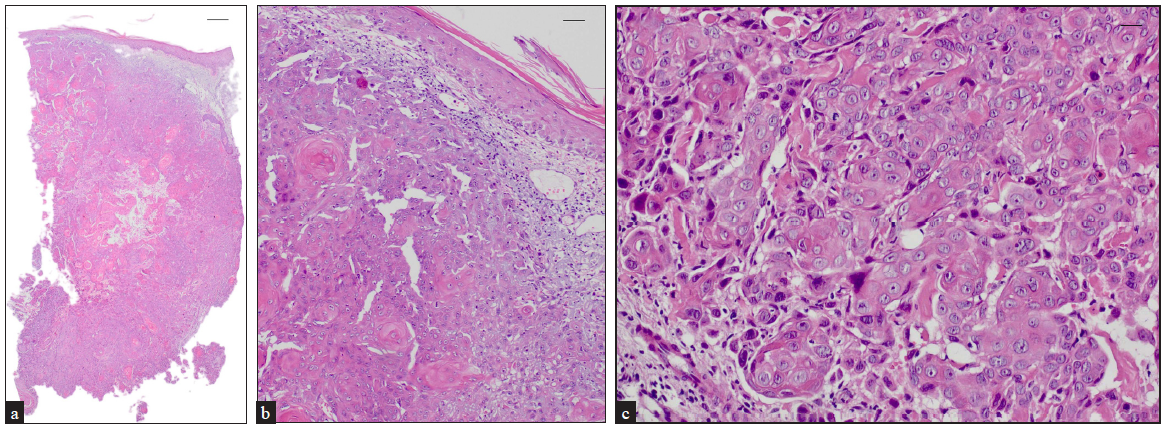
- Histological appearance of a satellite lesion. (a) Atypical squamous cell proliferation infiltrating the dermis (Haematoxylin-eosin, 20x); scale bar = 500 μm. (b) Higher magnification view showcasing the invasive character of the cell proliferation Haematoxylin-eosin, 100x); scale bar = 100 μm. (c) Moderate differentiation of tumoural cells (Haematoxylin-eosin, 200x); scale bar = 50 μm.

- Complete regression of tumoural lesion after 26 weeks.
This case illustrates the distinctive evolution of an advanced CSCC. In this scenario, the consideration of keratoacanthoma (KA) as an alternative diagnosis arises, given its propensity for self-regression.3,4 Although differentiating CSCC from KA may be challenging histologically, the size and macroscopic morphology of the main lesion and the satellites clearly suggest a primary tumour with regional progression.3–5
Spontaneous resolution (SR) is defined as a complete or partial regression of a malignant tumour in the absence of any treatment. The actual rate of SR cases among the general population remains unknown. Most reported cases are related to melanoma, non-small cell lung cancer, renal cell cancer, and neuroblastoma.6,7 In addition, there have been reports of metastatic squamous cell carcinoma with SR, particularly in the lung.8 The mechanisms behind SR are thought to include immune modulation in response to trauma or infection, hormonal and psychoneuroimmunological mechanisms.1,7,8
Cole et al. conducted a study of 176 cases of SR of cancer and proposed that stimulating factors, especially operative trauma (e.g., incisional biopsy), induce a systemic immunological response against tumour cells, involving both primary and metastatic lesions.7 Moreover, in our case, the patient also had a history of localised renal cell carcinoma that remained stable after the CSCC regression which suggests a possible CSCC-specific SR-mechanism.
So far, only four cases of SR of localised CSCC have been reported. In 1988, Roseman described a case where the surgical and radiotherapy treatment of a cutaneous metastasis resulted in a complete perdurable remission of the primary lesion.2 All these cases had a history of surgical trauma, mostly incisional biopsy.
To our knowledge, no previous studies have reported complete SR of metastatic CSCC without invasive treatments. Optimal follow-up protocols for these cases are unknown. However, close follow-up visits should be encouraged, given the likelihood of new neoplasms in areas of field cancerisation. Further studies are required to clarify the underlying mechanism that induces SR in advanced CSCC.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Cutaneous squamous cell carcinoma: From biology to therapy. Int J Mol Sci. 2020;21:2956.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Regression of locally recurrent squamous cell carcinoma of the skin following excision of a metastasis: With review of the literature. J Surg Oncol. 1988;39:213-4.
- [CrossRef] [PubMed] [Google Scholar]
- A clinical and biological review of keratoacanthoma. Br J Dermatol. 2021;185:487-98.
- [CrossRef] [PubMed] [Google Scholar]
- Giant keratoacanthoma: Case report and review of the english literature. Am J Dermatopathol. 2014;36:252.
- [CrossRef] [PubMed] [Google Scholar]
- Differentiating squamous cell carcinoma from keratoacanthoma using histopathological criteria. Is it possible? A study of 296 cases. Dermatol. 1999;199:208-12.
- [CrossRef] [PubMed] [Google Scholar]
- Spontaneous regression of cutaneous metastases of squamous cell carcinoma. QJM. 2014;107:61-3.
- [CrossRef] [PubMed] [Google Scholar]
- Efforts to explain spontaneous regression of cancer. J Surg Oncol. 1981;17:201-9.
- [CrossRef] [PubMed] [Google Scholar]
- Spontaneous regression in advanced non-small cell lung cancer. BMJ Case Rep. 2010;2010:bcr0720103147.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]




