
Translate this page into:
Squamoid eccrine ductal carcinoma: A frequently misdiagnosed entity
Corresponding author: Dr. Pooja Srivastava, Department of Pathology, University of Pittsburgh Medical Center, 3550 Terrace Street, Pittsburgh, PA, United States. panacea.2417@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Srivastava P, Dando E, Doeden K. Squamoid eccrine ductal carcinoma: A frequently misdiagnosed entity. Indian J Dermatol Venereol Leprol. 2024;90:503-5. doi: 10.25259/IJDVL_310_2022
Dear Editor,
Eccrine carcinomas comprise around 0.01% of all tumours.1 Squamoid eccrine ductal carcinoma (SEDC) is a rare tumour first described by Wong et al. in 1997, representing a lesion showing eccrine ductal differentiation along with a prominent squamous component.2 It usually involves the head and neck area and only few cases have been reported in the English literature, including a series of 30 patients by van der Horst et al.3 Accurate diagnosis is crucial given its aggressive nature, along with increased risk of local recurrence and metastasis.
An 89-year-old male presented to VA Medical Center, Pittsburgh with a non-healing lesion of unknown duration on right posterior shoulder. Clinical examination revealed a 2.0 × 1.0 cm ulcerated pink plaque with violaceous border [Figure 1]. Histopathology revealed epidermal ulceration with proliferation of infiltrating glandular structures composed of markedly pleomorphic squamoid cells containing intraluminal secretions [Figures 2a and 2b]. Abundant mitoses were noted, along with tumour cell necrosis and focal perineural invasion [Figure 2c]. On immunohistochemistry, the neoplastic cells were positive for CEA [Figure 3a], p63 [Figure 3b], CK5/6 and weakly positive for GATA3. Mucicarmine stain was negative. Based on morphology and immunohistochemistry, a diagnosis of squamoid eccrine ductal carcinoma was made. We recommended wide local excision, but the patient declined further management citing advanced age and medical comorbidities. He died two years later due to unrelated causes.

- Ulcerated pink plaque (2.0 × 1.0 cm) with violaceous border on the right posterior shoulder.
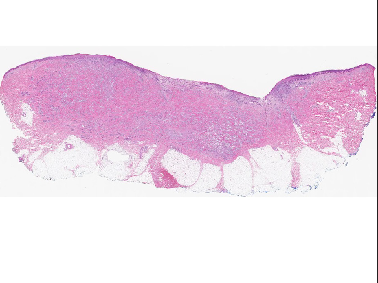
- Epidermal ulceration and proliferation of tumour cells within the dermis (Haematoxylin & Eosin, 20x).
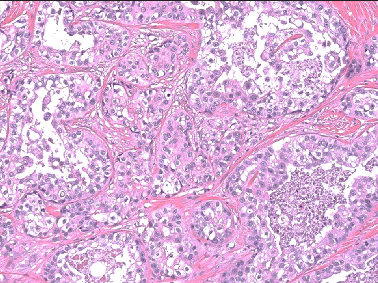
- Proliferation of infiltrating glandular structures within the dermis with ductal structures showing markedly pleomorphic squamoid cells (Haematoxylin & Eosin, 200x).
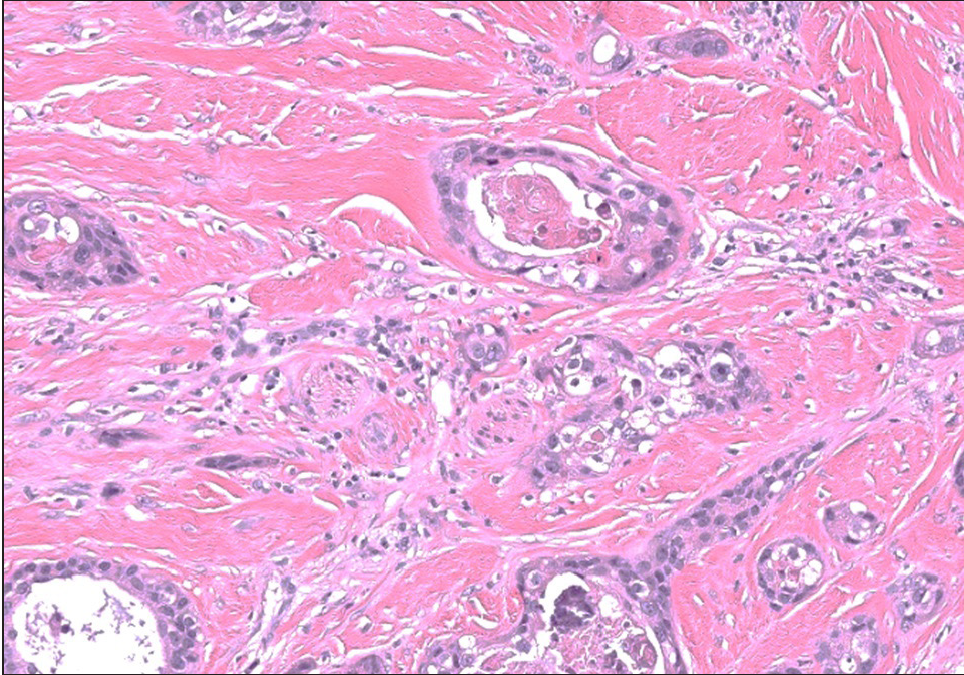
- Tumour cells with foci of intraluminal necrosis and perineural infiltration (Haematoxylin & Eosin, 200x)
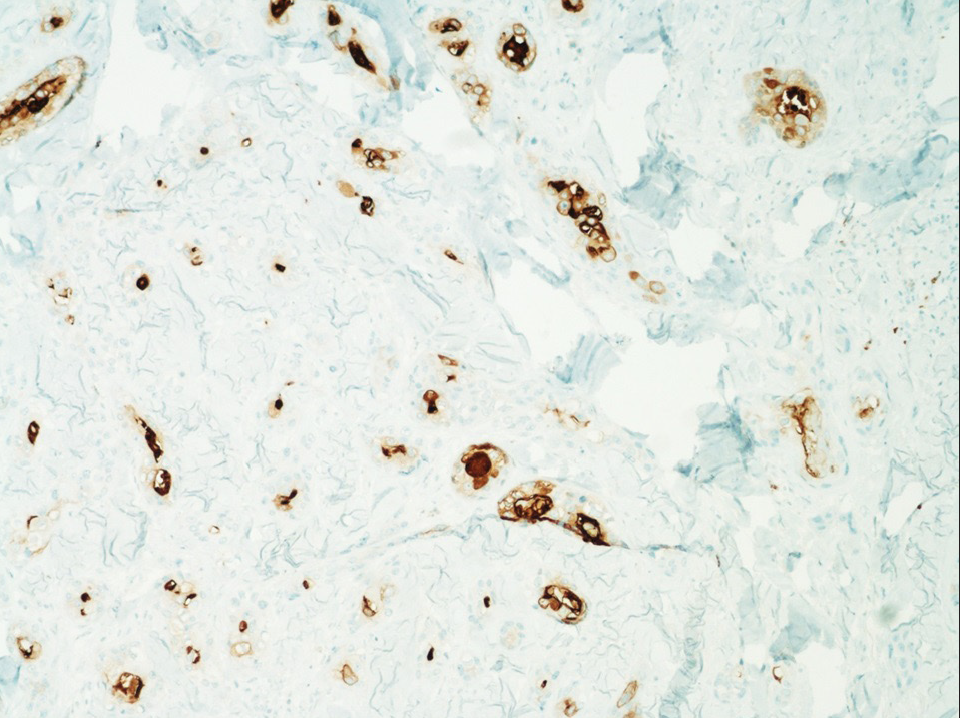
- CEA immunostaining showing intraluminal staining pattern within the tumour cells (IHC, 100x).
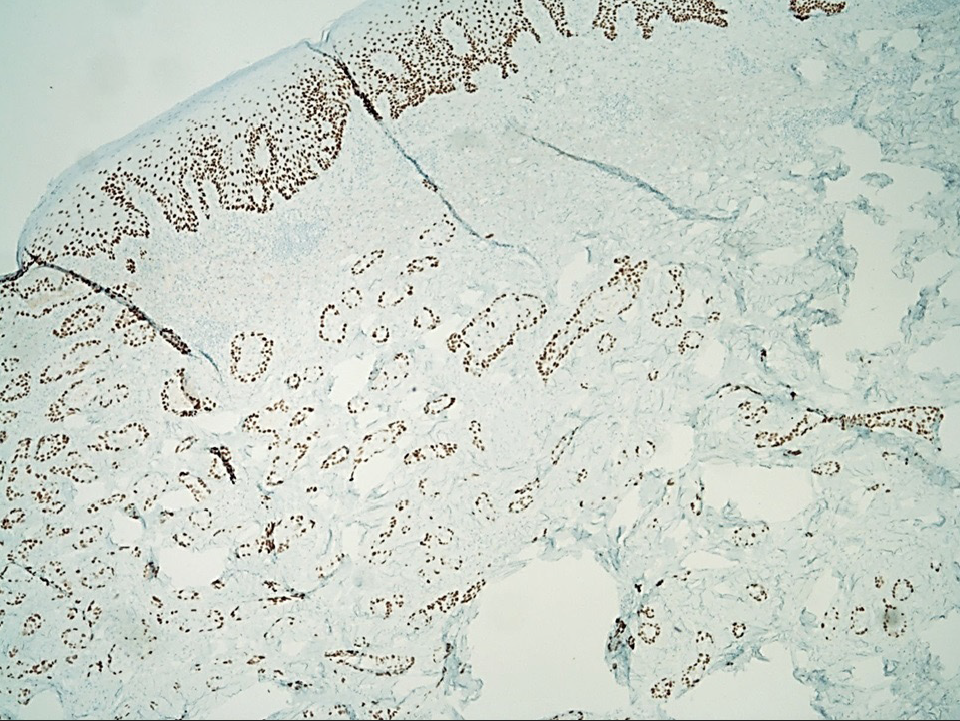
- p63 immunostain is positive in the tumour cells (IHC, 40x).
Squamoid eccrine ductal carcinoma is a rare eccrine carcinoma, commonly affecting the seventh to eighth decade (age range 30–91 years). There is slight male predominance and usually involves the head and neck as a slow-growing nodule or plaque with ulceration or crusting.2 Few cases have been reported in the extremities or trunk.3 Histologically, the tumour exhibits a biphasic growth pattern with the superficial component resembling squamous cell carcinoma (SCC) and the deeper component demonstrating ductal differentiation indicating eccrine ductal carcinoma.2,3 These tumours exhibit marked cytologic atypia with desmoplastic stroma and cords of deeply infiltrative tumour cells. Mitoses are frequent\along with perineural invasion. Rarely, tumoural necrosis and lymphovascular invasion may beobserved.
The histologic differentials include squamous cell carcinoma, porocarcinoma with squamous differentiation, microcystic adnexal carcinoma and cutaneous metastasis from visceral tumours.1 Adequate sampling and histologic examination are necessary to demonstrate ductal differentiation in the deeper component to rule out squamous cell carcinoma. Chhibber et al. reported a case of squamoid eccrine ductal carcinoma, repeatedly misdiagnosed as squamous cell carcinoma on biopsy.1
Porocarcinoma usually affects the lower extremity while squamoid eccrine ductal carcinoma predominantly involves the head and neck region. Porocarcinoma demonstrates tumour cells with poroid characteristics in a background of pre-existing poroma. Microcystic adnexal carcinoma usually shows both follicular and ductal differentiation with keratinous cystic structures the in superficial component, and small nests of cells, lacking significant cytologic atypia in the deeper component.3 p63 immunostain positivity favours a primary cutaneous sweat gland carcinoma over metastatic adenocarcinoma. EMA and CEA are typically positive in glandular tissue and usually negative in epithelial malignancies such as squamous cell carcinoma. Hence, their positivity indicates an adnexal origin.4 Like other eccrine carcinomas, squamoid eccrine ductal carcinoma may become aggressive. Among 24 patients followed-up by van der Horst et al., six (25%) developed local recurrence, three (12.5%) lymph node metastasis and one (4%) widespread systemic metastatic resulting in death.3 It is unclear whether further workup like sentinel lymph node biopsy or imaging is indicated, due to the rarity of this tumour and lack of randomized studies. There is no accepted standard margin for surgical resection. Recurrence may be minimized by Mohs micrographic surgery, compared to wide local excision. A literature review by Kim et al. reported local recurrence rates of 10–70% after wide local excision which reduced to 0–5% following Mohs micrographic surgery after ~30.9 months follow-up.5 Thus, these tumours require close clinical follow-up to avoid recurrence.
Squamoid eccrine ductal carcinoma is a diagnostic challenge, as it is an eccrine gland tumour histologically resembling squamous cell carcinoma superficially, and deeper tissue sampling is needed to reveal ductal differentiation. These deeply infiltrating tumours frequently demonstrate perineural invasion and are candidates for local recurrence and metastasis. Immunostaining with p63, EMA, CEA and mucicarmine may help in differentiating them from histologic mimics. Treatment with Mohs micrographic surgery ensures complete margin control, and is recommended to minimize local recurrence.
Declaration of patient consent
Patient’s consent not required as the patient’s identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Ductal eccrine carcinoma with squamous differentiation: Apropos a case. J Cutan Pathol. 2007;34:503-7.
- [CrossRef] [PubMed] [Google Scholar]
- Anatomoclinical study of 30 cases of sclerosing sweat duct carcinomas (microcystic adnexal carcinoma, syringomatous carcinoma and squamoid eccrine ductal carcinoma) J Eur Acad Dermatol Venereol. 2015;29:1978-94.
- [CrossRef] [PubMed] [Google Scholar]
- Squamoid eccrine ductal carcinoma: A clinicopathologic study of 30 cases. Am J Surg Pathol. 2016;40:755-60.
- [CrossRef] [PubMed] [Google Scholar]
- Squamoid eccrine ductal carcinoma: a case report and review of the literature. Am J Dermatopathol. 2010;32:287-92.
- [CrossRef] [PubMed] [Google Scholar]
- Mohs micrographic surgery for squamoid eccrine ductal carcinoma. Dermatol Surg. 2005;31:1462-4.
- [CrossRef] [PubMed] [Google Scholar]




