Translate this page into:
Squamous cell carcinoma in hypertrophic lichen planus
2 Consultant Dermatologist, B. S. E. S Hospital, Mumbai, India
Correspondence Address:
Rajiv Joshi
14 Jay Mahal, A Road, Churchgate, Mumbai - 400 020
India
| How to cite this article: Joshi R, Durve U. Squamous cell carcinoma in hypertrophic lichen planus. Indian J Dermatol Venereol Leprol 2007;73:54-55 |
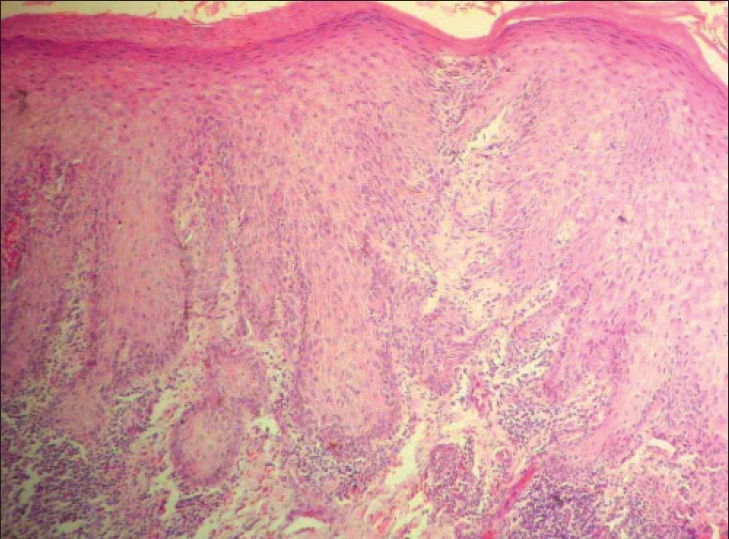 |
| Irregular epidermal hyperplasia with atypia (H/E, x200) |
|
| Irregular epidermal hyperplasia with atypia (H/E, x200) |
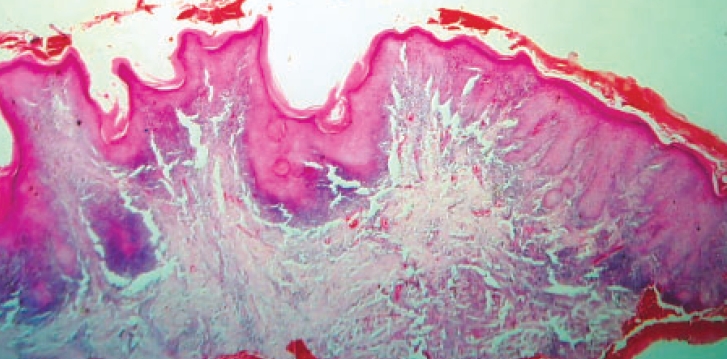 |
| Low-power view showing hypertrophic lichen planus on the left and squamous cell carcinoma on the right of the section (H/E, x100) |
|
| Low-power view showing hypertrophic lichen planus on the left and squamous cell carcinoma on the right of the section (H/E, x100) |
 |
| Large ulcer with everted margins and keratotic crusts |
|
| Large ulcer with everted margins and keratotic crusts |
Sir,
We read with interest the article "Malignant transformation of hypertrophic lichen planus" by Sengupta et al .[1] We had encountered a similar case of malignant transformation occurring in hypertrophic lichen planus.
Neoplastic transformation (development of squamous cell carcinoma / verrucous carcinoma) in lichen planus has been described, especially in the oral form of the disease where an estimated 0.3-3% of patients may develop squamous cell carcinoma.[2] Malignancy though uncommon with cutaneous lichen planus has been described in chronic hypertrophic lesions of lichen planus on the legs,[3],[4],[5] including a case of metastatic squamous cell carcinoma developing in a 34-year-old male in chronic hypertrophic lesions of lichen planus on the legs of more than 10 years duration.[6]
We describe a 25-year-old male who presented to one of us (UD) with a non-healing ulcer over the anterior aspect of the left leg just above the ankle of about four to five months duration [Figure - 1]. The ulcer was large, 4 cm in diameter and with a raised everted keratotic edge. The ulcer floor was hypertrophic, covered with slough and keratotic crusts; the lesion was friable and bled on manipulation. The surrounding skin was thickened, lichenified and pigmented. Both legs had postinflammatory changes at sites of earlier lesions. No significant inguinal lymphadenopathy was present.
He gave a history of multiple raised rough pruritic lesions on both the legs for several years and had been taking treatment off and on from several dermatologists for at least four years prior to this presentation. The earlier clinical diagnoses were chronic lichenified eczema and hypertrophic lichen planus; however, no biopsy had been done in the past. Previous treatments included topical betamethasone and salicylic acid with partial response.
A biopsy from the ulcer margin showed features of hypertrophic lichen planus towards one end of the section with hyperplastic follicular infundibula that showed interface changes and a lichenoid lympho-histiocytic infiltrate with melanophages at their bases [Figure - 2],[Figure - 3]. The other end of the section showed irregular hyperplasia of the epidermis with atypia of the lower epithelium and in the dermis showed an invasive squamous cell carcinoma with irregular jagged tongues of atypical epithelium infiltrating the dermal tissue [Figure 4],[Figure 5],[Figure 6]. A second biopsy from the ulcer floor showed a keratotic squamous cell carcinoma with horn pearl formation.
Development of squamous cell carcinoma in lesions of hypertrophic lichen planus has been described in Indians,[7],[8] as has been a case of squamous cell carcinoma developing in a plaque of lichen simplex chronicus.[9]
Hypertrophic lichen planus on the legs tends to persist and has a propensity for malignant transformation even in young patients. Therefore nonhealing ulcers overlying such lesions should be viewed with great suspicion and biopsy performed to rule out squamous cell carcinoma.
| 1. |
Sengupta S, Das JK, Gangopadhyay A. Malignant transformation of hypertrophic lichen planus. Indian J Dermatol Venereol Leprol 2006;72:470-470.
[Google Scholar]
|
| 2. |
Castano E, Lopez-Rios F, Alvarez-Fernandez JG, Rodriguez-Peralto JL, Iglesias L. Verrucous carcinoma in association with hypertrophic lichen planus. Clin Exp Dermatol 1997;22:23-5.
[Google Scholar]
|
| 3. |
Potter B, Fretzin D. Well differentiated epidermoid carcinoma arising in hypertrophic lichen planus. Arch Dermatol 1966,94:805-6.
[Google Scholar]
|
| 4. |
Gawkrodger DJ, Stephenson TJ, Thomas SE. Squamous cell carcinoma complicating lichen planus: A clinico-pathological study of three cases. Dermatology 1994;188:36-9.
[Google Scholar]
|
| 5. |
Manz B, Paasch U, Stierherling M. Squamous cell carcinoma as a complication of long standing hypertrophic lichen planus. Int J Dermatol 2005;44:773-4.
[Google Scholar]
|
| 6. |
Ardabili M, Gambicher T, Rotterdam S, Altmeyer P, Hoffmann K, Stucker M. Metastatic cutaneous squamous cell carcinoma arising from chronic hypertrophic lichen planus. Dermatol Online J 2003;9:10.
[Google Scholar]
|
| 7. |
Yesudian P, Rao R. Malignant transformation of hypertrophic lichen planus. Int J Dermatol 1985:24:177-8.
[Google Scholar]
|
| 8. |
Jayaraman M, Janaki VR, Yesudian P. Squamous cell carcinoma arising from hypertrophic lichen planus. Int J Dermatol 1995:34:70-1.
[Google Scholar]
|
| 9. |
Balachandran C, Ramnarayan K. Squamous cell carcinoma on preexisting plaque of lichen simplex chronicus. Indian J Dermatol Venereo Leprol 1994;60:219-20.
[Google Scholar]
|
Fulltext Views
3,164
PDF downloads
1,981





![[Figure - 1]](#fig_ijdvl_2007_73_1_54_30658_1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2007_73_1_54_30658_2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2007_73_1_54_30658_3.jpg){kind=link}