Translate this page into:
Squamous cell carcinoma presenting as a giant cutaneous horn of the lower lip
Correspondence Address:
Mirjana Popadić
Pasterova 2, 11000 Belgrade
Serbia
| How to cite this article: Popadić M. Squamous cell carcinoma presenting as a giant cutaneous horn of the lower lip. Indian J Dermatol Venereol Leprol 2014;80:74-76 |
Sir,
A 76-year-old Caucasian female was referred to the dermatology clinic because of an asymptomatic, solitary lesion located at the vermilion border of her lower lip near the right oral commissure. The lesion has been present for several years and gradually increasing in size reached the final size, from the base to the tip, of 6.3 cm and 1.9 cm in maximum circumference. She was a non-smoker with poor oral hygiene and with no history of significant sunlight exposure during her life. There was no history of previous trauma, spontaneous bleeding or ulceration. Clinical examination revealed an isolated, exophytic, sessile, hard and well-circumscribed keratinized lesion arising from the lower lip [Figure - 1]. There were no enlarged regional lymph nodes and she was in good health with no systemic symptoms. The clinical diagnosis of cutaneous horn was made. Complete excision was performed and histopathology revealed diffuse hyperkeratosis and parakeratosis, consistent with a cutaneous horn. At the base of lesion, there was a neoplastic proliferation of atypical keratinocytes with large hyperchromatic nuclei extending into the dermis [Figure - 2]. Pleomorphism of keratinocytes was mild to moderate (well-differentiated tumor), with plenty of mitotic figures [Figure - 3]. A diagnosis of invasive squamous cell carcinoma was made. Imaging and analytical studies revealed neither bony involvement nor metastatic disease. No clinical relapse has been observed after 37 months of follow-up.
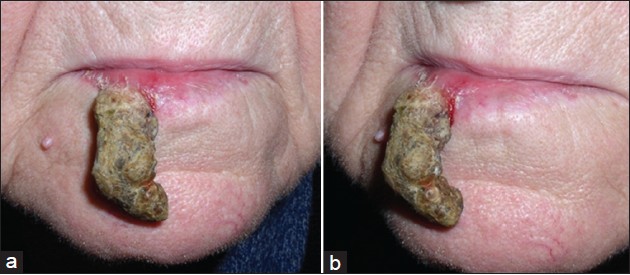 |
| Figure 1: Clinical images of cutaneous horn on the lower lip, front view (a) and profile (b). An isolated, exophytic, sessile, hard and well circumscribed keratinized lesion arising from the lower lip |
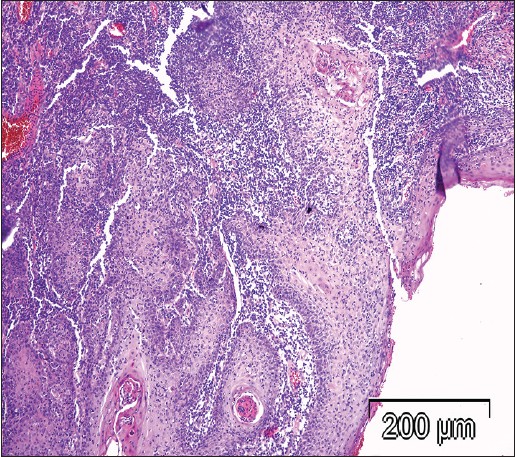 |
| Figure 2: Histopathological features of the tumor: The exophytic component of the tumor shows a papillary squamous cell carcinoma and the invasive component goes into a broad front in the tissue depth reaching the reticular dermis. It is composed of larger pale staining keratinocytes with scanty atypia. Many inflammatory cells (lymphocytes and plasma cells) infiltrate the papillary and reticular dermis (H and E, ×100) |
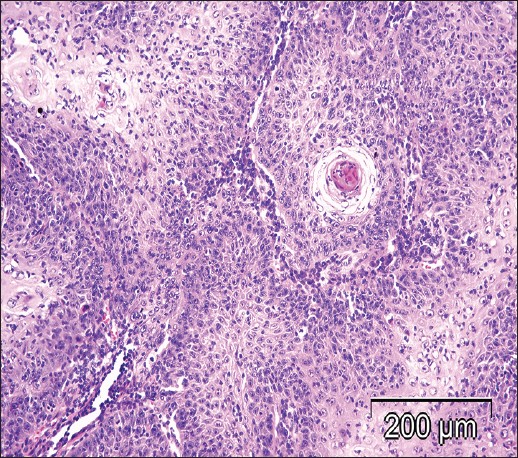 |
| Figure 3: Histopathological features of the tumor: Pleomorphism of keratinocytes is mild to moderate (well-differentiated tumor), with plenty of mitotic figures (H and E, ×200) |
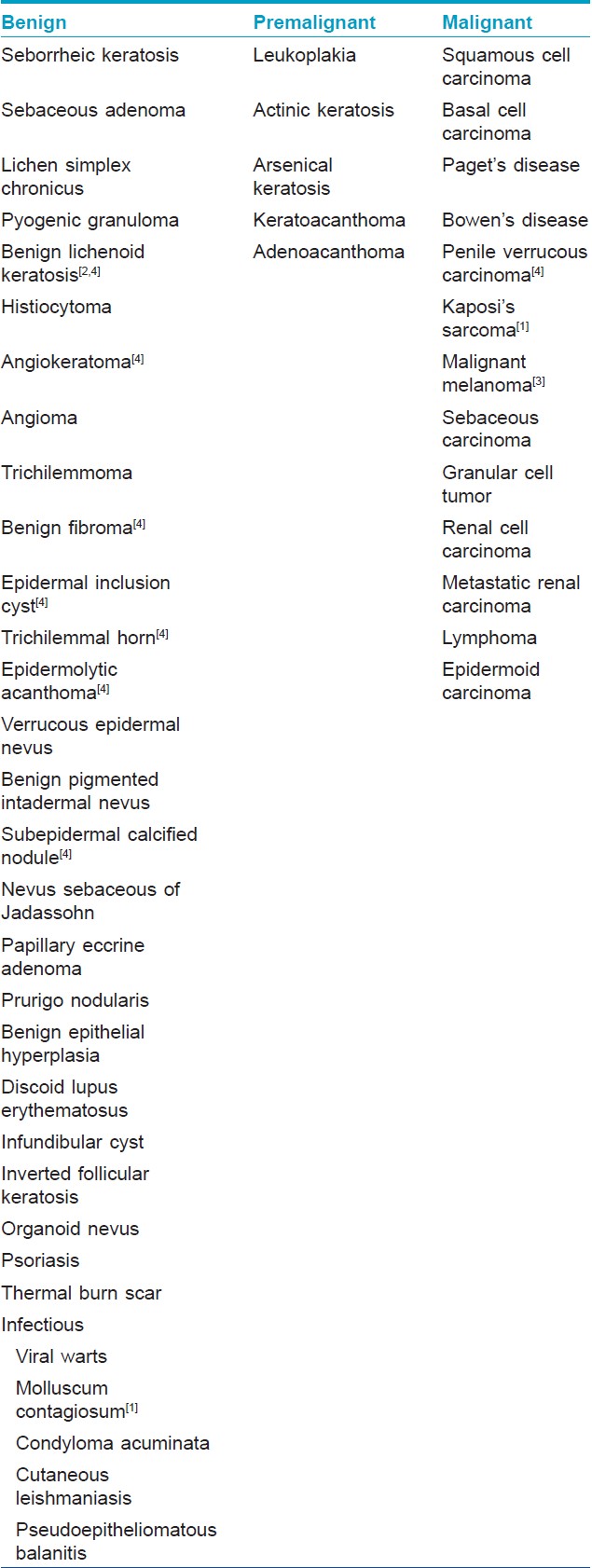
Cutaneous horn is a clinical term describing the characteristic conical shape of compact keratin that resembles a miniature animal horn. There are no available figures on the incidence and prevalence of cutaneous horns. One large histopathological analysis estimated the frequency to be 0.3-1.3%. [1] Sun exposure is the most important etiological factor in the pathogenesis of the cutaneous horn. However, poor oral hygiene and smoking may have an additional role in their development on the lips. Cutaneous horns are characterized by hyperproliferation and increased cohesiveness of keratin due to unknown mechanism [2] Clinical diagnosis of the pathology at the base may be difficult because cutaneous horns may mask numerous conditions producing a low level of diagnostic accuracy. Therefore, the important issue is not the horn itself, but rather the nature of the underlying disease [Table - 1]. Histopathological examination of the base of the lesion is, therefore, necessary to rule out cancer.
Risk factors of underlying malignancy include advanced age, male sex, large base or height-to-base ratio and location on sun-exposed areas. [1] Hardness at the base, the length of development, the history of trauma and the presence of other malignant lesions favor malignancy. [5] Large cutaneous horns, particularly giant horns, are considered to be commonly derived from malignant base. [5]
The reported incidence of cutaneous horns with premalignant or malignant histological features varies considerably. In the two largest published series, which included 634 and 514 patients with cutaneous horns, 38.9% and 74.6% of cases respectively were derived from malignant or premalignant epidermal lesions. [1] Another large study which included 230 cutaneous horns reported 58% of either premalignant or malignant changes at their base. [2] True malignancy underlying cutaneous horns was presented in 16-20% of cases, with squamous cell carcinoma being the most common type. [5] Therefore, adequate therapy requires wide excision with a tumor-free margin of at least 3 mm, particularly in the facial region where the incidence of malignancy is higher. [2],[5]
This article presents a case of giant cutaneous horn of the lower lip at an extremely rare location. There are no validated data on the prevalence and incidence of cutaneous horns occurring at this location. A literature review revealed only eight previous reports. [1],[2],[3],[4],[5] In three reports, the cutaneous horns originated from areas of leukoplakia. In two cases, the cutaneous horn developed from actinic keratoses and one each in pyogenic granuloma and keratoacanthoma. However, there was only one previous report of malignant transformation at the base. [4] This case is the longest cutaneous horn of the lips and the second labial horn infiltrated by squamous cell carcinoma at its base.
| 1. |
Yu RC, Pryce DW, Macfarlane AW, Stewart TW. A histopathological study of 643 cutaneous horns. Br J Dermatol 1991;124:449-52.
[Google Scholar]
|
| 2. |
Souza LN, Martins CR, de Paula AM. Cutaneous horn occurring on the lip of a child. Int J Paediatr Dent 2003;13:365-7.
[Google Scholar]
|
| 3. |
Stavroulaki P, Mal RK. Squamous cell carcinoma presenting as a cutaneous horn. Auris Nasus Larynx 2000;27:277-9.
[Google Scholar]
|
| 4. |
Skoulakis C, Theos E, Chlopsidis P, Manios AG, Feritsean A, Papadakis E. Giant cutaneous horn on squamous cell carcinoma of the lower lip. Eur J Plast Surg 2009;32:257-9.
[Google Scholar]
|
| 5. |
Mutaf M. A rare perioral lesion: Cutaneous horn of the lower lip. Eur J Plast Surg 2007;29:339-41.
[Google Scholar]
|
Fulltext Views
2,080
PDF downloads
1,409





![[Figure - 1]](#fig_ijdvl_2014_80_1_74_125469_u1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2014_80_1_74_125469_u2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2014_80_1_74_125469_u3.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2014_80_1_74_125469_b4.jpg){kind=link}