Translate this page into:
Steroid-resistant erythroderma and alopecia in a newborn
Correspondence Address:
Rana A El Khoury
Hotel-Dieu de France, Alfred Naccache Avenue, Achrafieh, Beirut
Lebanon
| How to cite this article: El Khoury RA, Maalouf EH, Kechichian EG, Tomb RR. Steroid-resistant erythroderma and alopecia in a newborn. Indian J Dermatol Venereol Leprol 2018;84:304-306 |
A 6-month-old girl presented to the emergency department, with complaints of irritability and decreased oral intake. The infant was born of a non-consanguineous marriage, at term, without any collodion membrane at birth. Her medical history included a generalized non-itchy, ill-defined, erythematous rash since the 1st week of life treated many times with topical steroids without any improvement, milk intolerance (vomiting without diarrhea), growth retardation and recurrent bacterial infections. On physical examination, the infant displayed signs of severe dehydration. Skin examination revealed a generalized eczematous rash exaggerated over periorificial and flexural areas without mucosal involvement [Figure - 1] as well as linear and serpiginous lesions with double-edged scaling on the lower limbs and trunk [Figure - 2]. She also had non-scarring alopecia of the scalp and eyebrows [Figure - 3]. Skin cultures from different sites revealed growth of methicillin-sensitive Staphylococcus aureus strains. Laboratory testing revealed high neutrophil counts and elevated inflammatory markers. Eosinophil counts, immunoglobulin levels and blood flow cytometry examination were within normal limits. Serum zinc and sodium were within normal range, 0.95 mcg/ml and 143 mEq/L, respectively. Biotin supplementation did not improve her skin condition. The trichogram of scalp hair and eyebrows is shown in [Figure - 4]. Her parents declined skin biopsy and genetic tests were not performed due to financial constraints.
 |
| Figure 1: Generalized eczematous rash exaggerated over periorificial and flexural areas |
 |
| Figure 2: Linear and serpiginous lesions with double-edged scaling on the right lower limb |
 |
| Figure 3: Nonscarring eyebrow alopecia |
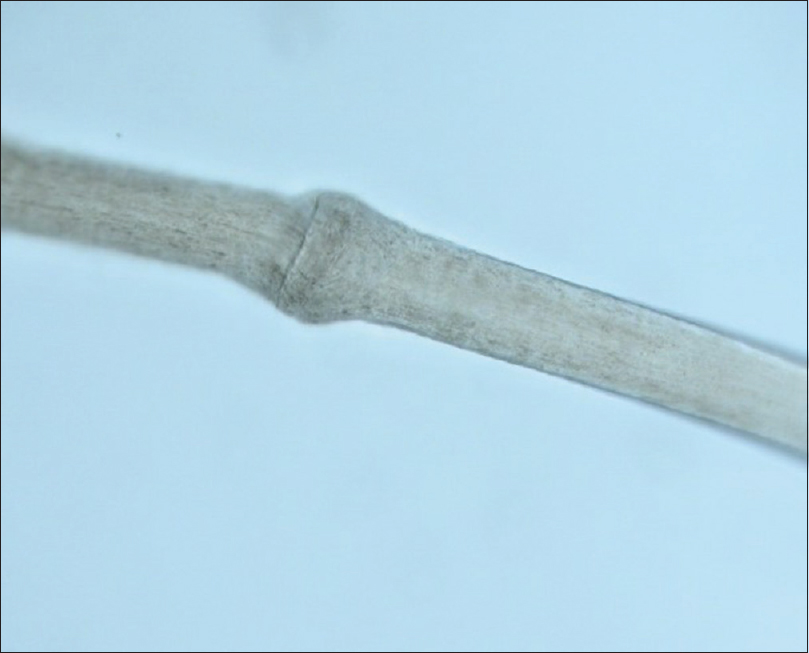 |
| Figure 4: Trichogram of scalp hair under optical microscopy with magnification 400x |
Question
What is your diagnosis?
Answer
Netherton syndrome.
Discussion
Comèl–Netherton syndrome is a rare, autosomal recessive genetic disorder, characterized by premature desquamation and thinning of the stratum corneum.[1] Diagnosis of Netherton syndrome is mainly clinical and is based on a triad of clinical signs. These signs include cutaneous features such as congenital ichthyosiform erythroderma or ichthyosis linearis circumflexa, hair shaft abnormalities including the pathognomonic finding of trichorrhexis invaginata or other less specific findings such as pili torti and trichorrhexis nodosa and atopic diathesis (asthma, urticaria, angioedema, allergic rhinitis, milk intolerance, high immunoglobulin E levels and hypereosinophilia).[1],[2],[3] Although genetic studies identified the responsible gene for this condition on chromosome 5q32, named serine protease inhibitor Kazal-type 5, which is responsible for encoding an inhibitor of serine proteases called lymphoepithelial Kazal-type-related inhibitor, genetic testing is not required yet to confirm the diagnosis.[1],[4] Despite advancements in clinical knowledge and molecular testing, diagnosing this disease is still challenging.[4]
The differential diagnosis of an erythemato-squamous rash in infants includes physiologic scaling and redness, psoriasis, seborrheic or atopic dermatitis, scabies, immunodeficiency, ectodermal dysplasias, acrodermatitis enteropathica and Netherton syndrome. The syndrome is under-recognized in the neonatal period with only 40% of cases being accurately diagnosed.[5] Exfoliative dermatitis often manifests 1–2 days after birth and can persist or progress to ichthyosis linearis circumflexa at the age of 1–2 years.[2],[6] Newborns and small infants typically present with nonbullous congenital ichthyosiform erythroderma, while ichthyosis linearis circumflexa is more common in the older child.[5] Ichthyosis linearis circumflexa can be the only clinical manifestation of Netherton syndrome.[5]
Alopecia is reported in one-third of children.[5] Skin findings together with skin biopsy and hair shaft examination are required to make the correct diagnosis. Histology is not specific and may reveal features of psoriasis or atopic dermatitis. Trichorrhexis invaginata is a pathognomonic feature and can confirm the diagnosis of Netherton syndrome.[1],[3] “Bamboo hair” affects only 20%–50% of the hairs; it may not appear before 1 year of age. Eyebrow examination can be helpful as they are involved early in life.[2] Trichorrhexis nodosa and pili torti may also occur.
Extracutaneous manifestations include enteropathy, hypoalbuminemia, aminoaciduria, mental retardation, growth retardation and impaired immunity of unknown origin.[2] In fact, gastrointestinal involvement is considered the second most prevalent manifestation after skin involvement (66% of children).[5] Growth retardation is present in more than 50% and up to 100% of cases.[5] It is caused by various infections and food allergies (cow milk, egg white, peanuts, wheat and fish).[2],[5] The potentially fatal immune deficiency is due to low antibody production, decreased activity of natural killers cells and proinflammatory cytokines. Susceptibility to develop S. aureus skin infections and sepsis are described in more than half of the cases.[5]
Treatment is only symptomatic, as a cure for the disease may not be possible. It relies on emollients along with topical steroids, as per need and oral vitamin A derivatives for transient effects. Spontaneous remission of the hair changes is possible and may occur at a later age. Narrowband ultraviolet B phototherapy is also useful for managing ichthyosis linearis circumflexa.[7]
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the legal guardian has given his consent for images and other clinical information to be reported in the journal. The guardian understands that names and initials will not be published and due efforts will be made to conceal patient identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Boskabadi H, Maamouri G, Mafinejad S. Netherton syndrome, a case report and review of literature. Iran J Pediatr 2013;23:611-2.
[Google Scholar]
|
| 2. |
Van Gysel D, Koning H, Baert MR, Savelkoul HF, Neijens HJ, Oranje AP. Clinico-immunological heterogeneity in Comèl-Netherton syndrome. Dermatology 2001;202:99-107.
[Google Scholar]
|
| 3. |
Hannula-Jouppi K, Laasanen SL, Heikkilä H, Tuomiranta M, Tuomi ML, Hilvo S, et al. IgE allergen component-based profiling and atopic manifestations in patients with Netherton syndrome. J Allergy Clin Immunol 2014;134:985-8.
[Google Scholar]
|
| 4. |
Bittencourt Mde J, Moure ER, Pies OT, Mendes AD, Deprá MM, Mello AL. Trichoscopy as a diagnostic tool in trichorrhexis invaginata and Netherton syndrome. An Bras Dermatol 2015;90:114-6.
[Google Scholar]
|
| 5. |
Sun JD, Linden KG. Netherton syndrome: A case report and review of the literature. Int J Dermatol 2006;45:693-7.
[Google Scholar]
|
| 6. |
Malakar S, Lahiri K, Sengupta SR. Ichthyosis linearis circumflexa. Indian J Dermatol Venereol Leprol 1996;62:379-80.
[Google Scholar]
|
| 7. |
Riyaz N, Riyaz A. Erythematous polycyclic patches. Indian J Dermatol Venereol Leprol 2006;72:398.
[Google Scholar]
|
Fulltext Views
3,960
PDF downloads
3,867





![[Figure - 1]](#fig_ijdvl_2018_84_3_304_213435_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2018_84_3_304_213435_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2018_84_3_304_213435_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2018_84_3_304_213435_f4.jpg){kind=link}