Translate this page into:
Subcutaneous human dirofilariasis
2 Department of Microbiology, Kozhikode, Kerala, India
3 Department of Radiodiagnosis, Kozhikode, Kerala, India
4 Government Medical College, Kozhikode, Kerala, India
Correspondence Address:
Binitha Manikoth Payyanadan
Haritha, Beypore post, Kozhikode
India
| How to cite this article: Sukumarakurup S, Payyanadan BM, Mariyath R, Nagesh M, Moorkoth AP, Ellezhuthil D. Subcutaneous human dirofilariasis. Indian J Dermatol Venereol Leprol 2015;81:59-61 |
Sir,
We present a case of human subcutaneous dirofilariasis, a zoonosis of clinical importance. Dirofilariasis is a potentially fatal infection in dogs and certain other animals. Accidental infection occurs in humans due to bites from mosquitoes carrying the infective microfilariae. Human ocular and pulmonary dirofilariasis are more common than subcutaneous involvement. We report a case to focus attention on this rare cause of a subcutaneous nodule which is often misdiagnosed or overlooked.
In December 2013, a 40-year-old carpenter presented to our tertiary care center in Kerala with a painful swelling over the right side of his abdomen, present since 2 weeks. There was no history of contact with dogs or other animals.
On dermatological examination, there was a tender, inflamed erythematous plaque 10 × 6 cm in size, on the right flank. He was started on 500 mg of oral ampicillin-cloxacillin capsules 6-hourly. On the second day, the erythema and edema had subsided and a linear nodule was visible at the site [Figure - 1].
Routine blood and urine tests, absolute eosinophil count and serum IgE levels were within normal limits, and an HIV antibody test was negative. An ultrasound scan of the affected soft tissue revealed a continuously moving worm seen as thin parallel hyperechoic lines, surrounded by a thick hypoechoic area representing the coiled up worm and the surrounding granuloma, respectively [[Figure - 2]a].
 |
| Figure 1: Linear nodule on the right flank |
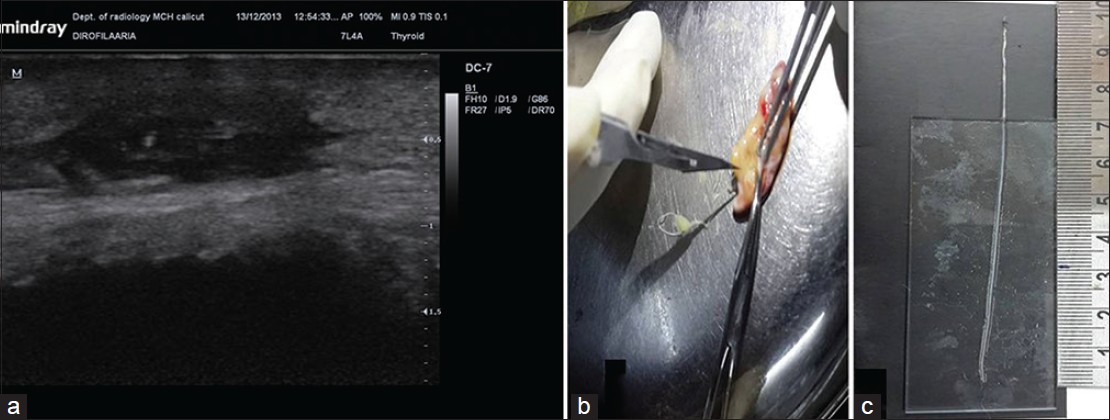 |
| Figure 2: (a) Ultrasonogram of the worm within the soft tissue. (b,c) The excised white, thread-like worm measuring 10 cm in length |
The patient was referred to the general surgery department and the mass was excised under local anaesthesia. Dissection of the excised subcutaneous tissue revealed a dead, white, thread-like worm which was 10 cm in length and 0.5 mm in width [[Figure - 2]b and c]. On gross microscopy, the worm had a thick cuticle and longitudinal wavy ridges with cross-striations, resulting in a beaded appearance [Figure - 3]. Histopathological examination showed a multi-layered cuticle, sections of longitudinal ridges and lateral chords typical of Dirofilaria repens. The cross section of the body cavity showed an intestinal tubule and a single reproductive tubule containing spermatocytes, indicating that it was a male worm [[Figure - 4]a and b].
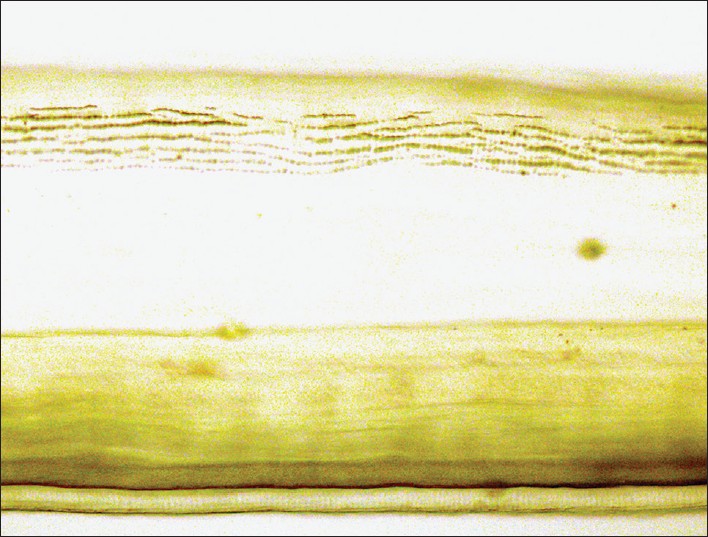 |
| Figure 3: Long, wavy ridges with cross-striations (computer-enhanced) on the thick cuticle.(x10) |
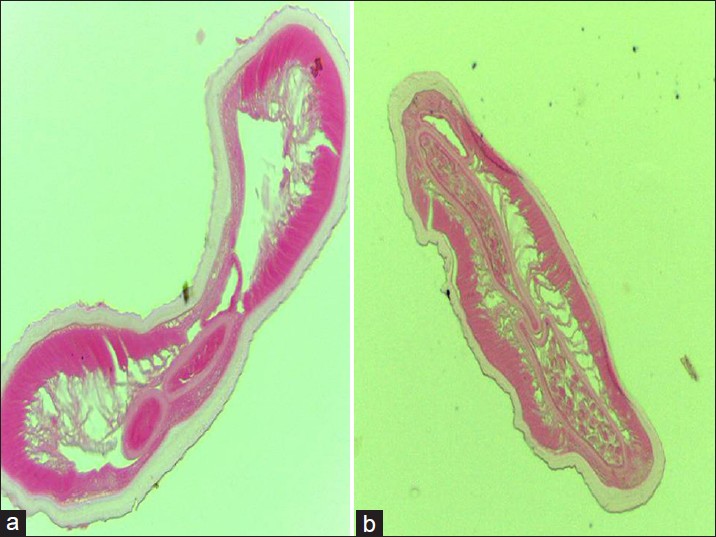 |
| Figure 4: Cross-section of the body cavity. (a) Multi-layered cuticle, section of longitudinal ridges, and lateral chords suggestive of D. repens and (b) section of intestinal and reproductive tubules |
The patient recovered rapidly and completely without any further treatment. He has been on monthly follow-up for the past ten months, without any signs of recurrence.
Various species of dirofilaria infect dogs, cats and other animals. These include D. immitis and D. repens (affecting dogs and cats), D. tenuis (raccoons) and D. ursi (bears). D. repens is the most commonly reported species causing human subcutaneous infection in Asia. [1] Microfilariae produced by the adult female worm circulate in the blood of the animal host, and are transformed into larvae within mosquitoes feeding on the infected animal. Humans are infected through bites of infected mosquitoes of genus Culex, Aedes or Anopheles. Culex pipiens was found to be the most common vector for D. immitis in a study in Italy. [2] Other vectors like fleas, lice and ticks may also transmit the infection. [3] The disease is self-limited as the parasite is unable to complete its life-cycle in the human host. Infections with female worms are three times more common than infections with male worms. [1] Very rarely, microfilariae have been demonstrated in human tissue, indicating that the gravid female worm can reproduce in human tissue. [4] However, detection of microfilaria in the peripheral blood is extremely rare ],[[4] and transmission of the disease from the human host has not been reported.
Subcutaneous infection may be under-reported as the condition usually subsides without treatment. [5] Ocular involvement is more commonly reported, [5] probably because eye lesions are more noticeable and produce more symptoms. The worm may be located in the subconjunctival, periorbital, periocular or intraocular regions. Ocular dirofilariasis is mostly due to D. repens and sometimes due to D. tenuis. Pulmonary involvement may also occur, usually caused by D. immitis, and presents with cough, wheezing, chest pain, hemoptysis or pleural effusion. Coin lesions of the lung may be seen on chest X-rays, mimicking malignancies.
Since only isolated case reports of human subcutaneous dirofilariasis are available, we present this case to create awareness about the condition, which should be considered in any patient presenting with an acute or chronic, single, often asymptomatic, subcutaneous nodule. This is especially significant because of the world-wide distribution of the nematode and the frequent absence of a history of contact with animals. Though it often resolves spontaneously, surgical removal is recommended for persistent lesions, resulting in an excellent outcome.
Acknowledgement
We thank Dr. Arun Zachariah, BVSc and AH, MS (wild animal health), Assistant Forest Veterinary Officer, Wildlife Disease Research Laboratory, Wayanad Wildlife Sanctuary, for his invaluable help.
| 1. |
Kotigadde S, Ramesh SA, Medappa KT. Human dirofilariasis due to Dirofilaria repens in southern India. Trop Parasitol 2012;2:67-8.
[Google Scholar]
|
| 2. |
Capelli G, Frangipane di Regalbono A, Simonato G, Cassini R, Cazzin S, Canerini G, et al. Risk of canine and human exposure to Dirofilaria immitis infected mosquitoes in endemic areas of Italy. Parasit Vectors 2013;6:60.
[Google Scholar]
|
| 3. |
Joseph E, Mathai A, Abraham LK, Thomas S. Subcutaneous human dirofilariasis. J Parasit Dis 2011;35:140-3.
[Google Scholar]
|
| 4. |
Orihel TC, Eberhard ML. Zoonotic filariasis. Clin Microbiol Rev 1998;11:366-81.
[Google Scholar]
|
| 5. |
Sanjeev H, Rajini M, Prasad SR. Human dirofilariasis: An uncommon case of subcutaneous infection with dirofilaria repens with a brief review of literature. Nitte Univ J Health Sci 2011;1:60-2.
[Google Scholar]
|
Fulltext Views
5,839
PDF downloads
3,764





![[Figure - 1]](#fig_ijdvl_2015_81_1_59_148576_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2015_81_1_59_148576_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2015_81_1_59_148576_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2015_81_1_59_148576_f4.jpg){kind=link}